Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women's Hospital and Harvard Medical School, Boston, Massachusetts, United States of America.
Office of Surveillance and Epidemiology, Center for Drug Evaluation and Research, Food and Drug Administration, Silver Spring, Maryland, United States of America.
PLoS Med. 2019 Mar 13;16(3):e1002763. doi: 10.1371/journal.pmed.1002763. eCollection 2019 Mar.
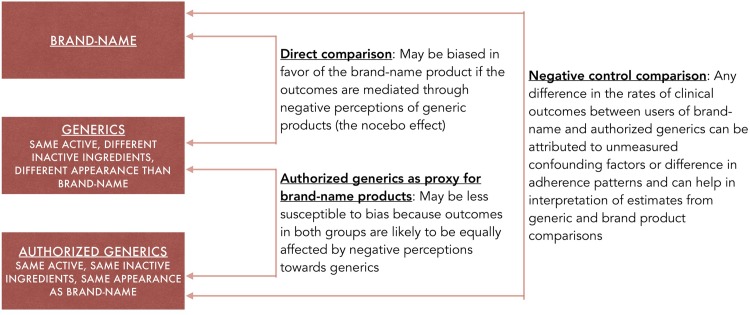
To the extent that outcomes are mediated through negative perceptions of generics (the nocebo effect), observational studies comparing brand-name and generic drugs are susceptible to bias favoring the brand-name drugs. We used authorized generic (AG) products, which are identical in composition and appearance to brand-name products but are marketed as generics, as a control group to address this bias in an evaluation aiming to compare the effectiveness of generic versus brand medications.
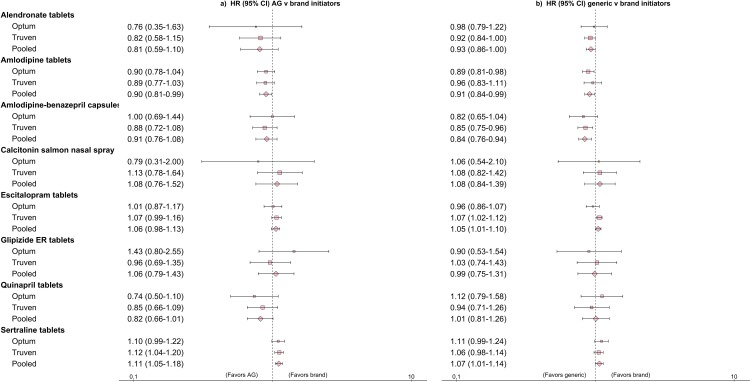
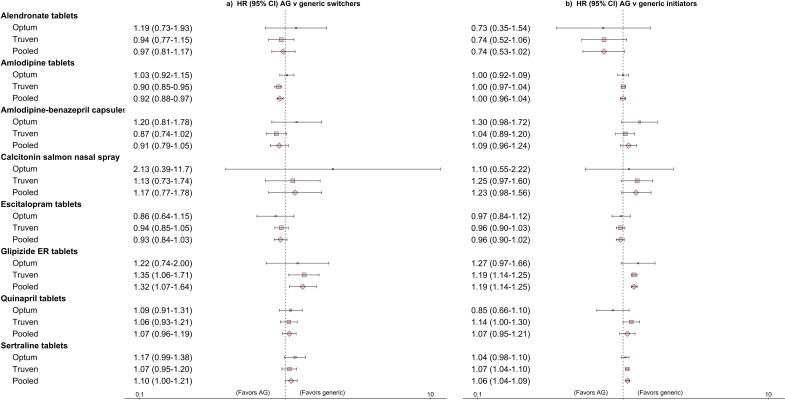
For commercial health insurance enrollees from the US, administrative claims data were derived from 2 databases: (1) Optum Clinformatics Data Mart (years: 2004-2013) and (2) Truven MarketScan (years: 2003-2015). For a total of 8 drug products, the following groups were compared using a cohort study design: (1) patients switching from brand-name products to AGs versus generics, and patients initiating treatment with AGs versus generics, where AG use proxied brand-name use, addressing negative perception bias, and (2) patients initiating generic versus brand-name products (bias-prone direct comparison) and patients initiating AG versus brand-name products (negative control). Using Cox proportional hazards regression after 1:1 propensity-score matching, we compared a composite cardiovascular endpoint (for amlodipine, amlodipine-benazepril, and quinapril), non-vertebral fracture (for alendronate and calcitonin), psychiatric hospitalization rate (for sertraline and escitalopram), and insulin initiation (for glipizide) between the groups. Inverse variance meta-analytic methods were used to pool adjusted hazard ratios (HRs) for each comparison between the 2 databases. Across 8 products, 2,264,774 matched pairs of patients were included in the comparisons of AGs versus generics. A majority (12 out of 16) of the clinical endpoint estimates showed similar outcomes between AGs and generics. Among the other 4 estimates that did have significantly different outcomes, 3 suggested improved outcomes with generics and 1 favored AGs (patients switching from amlodipine brand-name: HR [95% CI] 0.92 [0.88-0.97]). The comparison between generic and brand-name initiators involved 1,313,161 matched pairs, and no differences in outcomes were noted for alendronate, calcitonin, glipizide, or quinapril. We observed a lower risk of the composite cardiovascular endpoint with generics versus brand-name products for amlodipine and amlodipine-benazepril (HR [95% CI]: 0.91 [0.84-0.99] and 0.84 [0.76-0.94], respectively). For escitalopram and sertraline, we observed higher rates of psychiatric hospitalizations with generics (HR [95% CI]: 1.05 [1.01-1.10] and 1.07 [1.01-1.14], respectively). The negative control comparisons also indicated potentially higher rates of similar magnitude with AG compared to brand-name initiation for escitalopram and sertraline (HR [95% CI]: 1.06 [0.98-1.13] and 1.11 [1.05-1.18], respectively), suggesting that the differences observed between brand and generic users in these outcomes are likely explained by either residual confounding or generic perception bias. Limitations of this study include potential residual confounding due to the unavailability of certain clinical parameters in administrative claims data and the inability to evaluate surrogate outcomes, such as immediate changes in blood pressure, upon switching from brand products to generics.
In this study, we observed that use of generics was associated with comparable clinical outcomes to use of brand-name products. These results could help in promoting educational interventions aimed at increasing patient and provider confidence in the ability of generic medicines to manage chronic diseases.
由于结果受到对仿制药的负面看法(反安慰剂效应)的影响,因此比较品牌名药物和仿制药的观察性研究容易受到偏向品牌药物的偏见。我们使用授权仿制药(AG)作为对照组来解决这种偏见,这些药物在组成和外观上与品牌产品相同,但作为仿制药销售,用于评估比较仿制药与品牌药物的疗效。
对于来自美国的商业健康保险参保人,从 2 个数据库中获得了行政索赔数据:(1)Optum Clinformatics Data Mart(年份:2004-2013)和(2)Truven MarketScan(年份:2003-2015)。对于总共 8 种药物产品,使用队列研究设计比较了以下组:(1)从品牌药物转换为 AG 药物的患者与使用仿制药的患者,以及使用 AG 药物的患者与使用仿制药的患者,其中 AG 药物的使用代表了品牌药物的使用,解决了负面认知偏见,以及(2)使用仿制药的患者与使用品牌药物的患者(易产生偏见的直接比较)和使用 AG 药物的患者与使用品牌药物的患者(负向对照)。在 1:1 倾向评分匹配后使用 Cox 比例风险回归,我们比较了复合心血管终点(用于氨氯地平、氨氯地平-贝那普利和喹那普利)、非椎骨骨折(用于阿仑膦酸钠和降钙素)、精神病住院率(用于舍曲林和依西酞普兰)和胰岛素起始(用于格列吡嗪)。使用逆方差荟萃分析方法,对来自 2 个数据库的每组比较计算了调整后的风险比(HR)。在 8 种药物中,纳入了 2264774 对接受 AG 药物与仿制药比较的匹配患者。大多数(16 项中的 12 项)临床终点估计结果表明 AG 药物与仿制药之间的结果相似。在其他 4 项具有显著不同结果的估计中,有 3 项表明仿制药的结果更好,1 项有利于 AG 药物(从氨氯地平品牌药物转换的患者:HR[95%CI]0.92[0.88-0.97])。在仿制药和品牌药物启动者的比较中,涉及 1313161 对匹配患者,阿仑膦酸钠、降钙素、格列吡嗪或喹那普利的结果没有差异。与品牌药物相比,我们观察到氨氯地平和氨氯地平-贝那普利(HR[95%CI]0.91[0.84-0.99]和 0.84[0.76-0.94])以及阿仑膦酸钠和降钙素(HR[95%CI]0.91[0.84-0.99]和 0.84[0.76-0.94])的复合心血管终点风险较低。与品牌药物相比,我们观察到舍曲林和依西酞普兰的精神病住院率更高(HR[95%CI]1.05[1.01-1.10]和 1.07[1.01-1.14])。阴性对照比较还表明,与品牌药物启动相比,AG 药物的发生率可能更高(HR[95%CI]1.06[0.98-1.13]和 1.11[1.05-1.18]),表明这些结果中品牌药物使用者和仿制药使用者之间的差异可能是由残留混杂因素或仿制药认知偏见引起的。本研究的局限性包括行政索赔数据中某些临床参数的缺失可能导致潜在的残留混杂,以及无法评估替代结局,例如从品牌产品转换为仿制药后血压的即时变化。
在这项研究中,我们观察到使用仿制药与使用品牌药物的临床结果相当。这些结果有助于促进教育干预措施,旨在提高患者和提供者对治疗慢性疾病的通用药物的能力的信心。