University of Strathclyde, Department of Management Science, Glasgow, G4 0QU, Scotland, United Kingdom.
West of Scotland Pancreatic Cancer Unit, Glasgow Royal Infirmary, Glasgow, G4 0SF, Scotland, United Kingdom.
Sci Rep. 2019 Mar 13;9(1):4354. doi: 10.1038/s41598-019-40951-6.
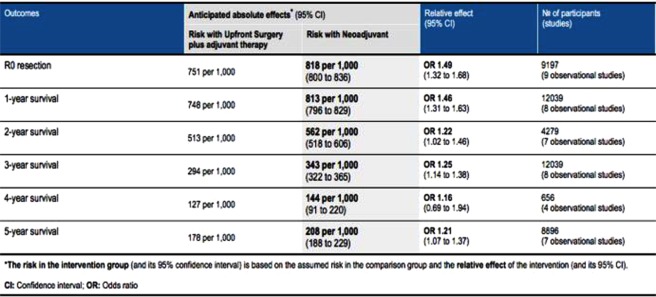
Current treatment recommendations for resectable pancreatic cancer support upfront resection and adjuvant therapy. Randomized controlled trials offering comparison with the emerging neoadjuvant approach are lacking. This review aims to compare both treatment strategies for resectable pancreatic cancer. PubMed, MEDLINE, Embase, Cochrane Database and Cochrane Databases were searched for studies comparing neoadjuvant and surgery-first with adjuvant therapy for resectable pancreatic cancer. A Bayesian network meta-analysis was conducted using the Markov chain Monte Carlo method. Cochrane Collaboration's risk of bias, ROBINS-I and GRADE tools were used to assess quality and risk of bias of included trials. 9 studies compared neoadjuvant therapy and surgery-first with adjuvant therapy (n = 22,285). Aggregate rate (AR) of R0 resection for neoadjuvant therapy was 0.8008 (0.3636-0.9144) versus 0.7515 (0.2026-0.8611) odds ratio (O.R.) 1.27 (95% CI 0.60-1.96). 1-year survival AR for neoadjuvant therapy was 0.7969 (0.6061-0.9500) versus 0.7481 (0.4848-0.8500) O.R. 1.38 (95% CI 0.69-2.96). 2-year survival AR for neoadjuvant therapy was 0.5178 (0.3000-0.5970) versus 0.5131 (0.2727-0.5346) O.R. 1.26 (95% CI 0.94-1.74). 5-year AR survival for neoadjuvant therapy was 0.2069 (0.0323-0.3300) versus 0.1783 (0.0606-0.2300) O.R. 1.19 (95% CI 0.65-1.73). In conclusion neoadjuvant therapy may offer benefit over surgery-first and adjuvant therapy. However, further randomized controlled trials are needed.
目前,可切除胰腺癌的治疗推荐方案支持进行术前切除和辅助治疗。缺乏与新兴新辅助方法进行比较的随机对照试验。本综述旨在比较可切除胰腺癌的两种治疗策略。使用 PubMed、MEDLINE、Embase、Cochrane 数据库和 Cochrane 数据库检索了比较新辅助治疗与手术优先加辅助治疗可切除胰腺癌的研究。使用 Markov 链蒙特卡罗方法进行贝叶斯网络荟萃分析。使用 Cochrane 协作的偏倚风险、ROBINS-I 和 GRADE 工具评估纳入试验的质量和偏倚风险。9 项研究比较了新辅助治疗与手术优先加辅助治疗(n=22285)。新辅助治疗的 R0 切除总率(AR)为 0.8008(0.3636-0.9144),而手术优先加辅助治疗的 AR 为 0.7515(0.2026-0.8611),比值比(OR)为 1.27(95%CI 0.60-1.96)。新辅助治疗的 1 年生存率 AR 为 0.7969(0.6061-0.9500),而手术优先加辅助治疗的 AR 为 0.7481(0.4848-0.8500),OR 为 1.38(95%CI 0.69-2.96)。新辅助治疗的 2 年生存率 AR 为 0.5178(0.3000-0.5970),而手术优先加辅助治疗的 AR 为 0.5131(0.2727-0.5346),OR 为 1.26(95%CI 0.94-1.74)。新辅助治疗的 5 年生存率 AR 为 0.2069(0.0323-0.3300),而手术优先加辅助治疗的 AR 为 0.1783(0.0606-0.2300),OR 为 1.19(95%CI 0.65-1.73)。总之,新辅助治疗可能比手术优先加辅助治疗更有益。然而,还需要进一步的随机对照试验。