Department of Gynecologic Oncology and Reproductive Medicine, Division of Surgery, The University of Texas MD Anderson Cancer Center, Houston, TX, United States of America.
Department of Health Services Research, The University of Texas MD Anderson Cancer Center, Houston, TX, United States of America.
Gynecol Oncol. 2019 Mar;152(3):439-444. doi: 10.1016/j.ygyno.2018.11.005.
To assess treatment patterns, outcomes, and costs for women with low-(LIR) and high-intermediate risk endometrial cancer (HIR) who are treated with and without adjuvant radiotherapy.
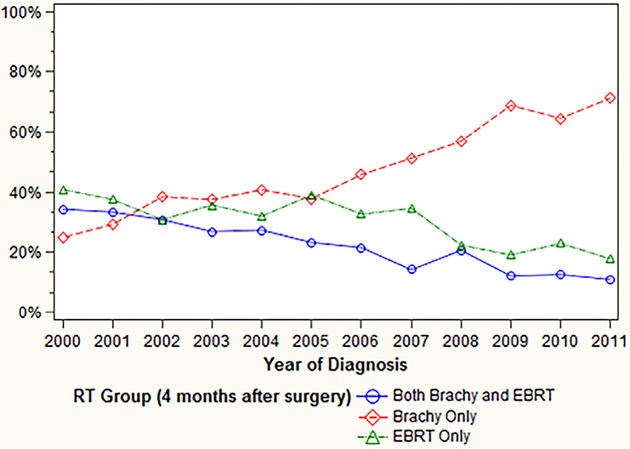
All patients with stage I endometrioid endometrial cancer who underwent surgery from 2000 to 2011 were identified from the SEER-Medicare database. LIR was defined as G1-2 tumors with <50% myometrial invasion or G3 with no invasion. HIR was defined as G1-2 tumors with ≥50% or G3 with <50% invasion. Patients were categorized according to whether they received adjuvant radiotherapy (vaginal brachytherapy [VBT], external beam radiotherapy [EBRT], or both) or no radiotherapy. Outcomes were analyzed and compared (primary outcome was overall survival).
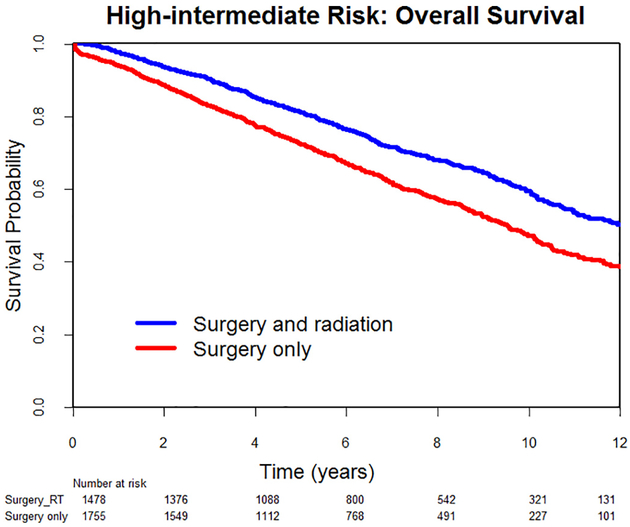
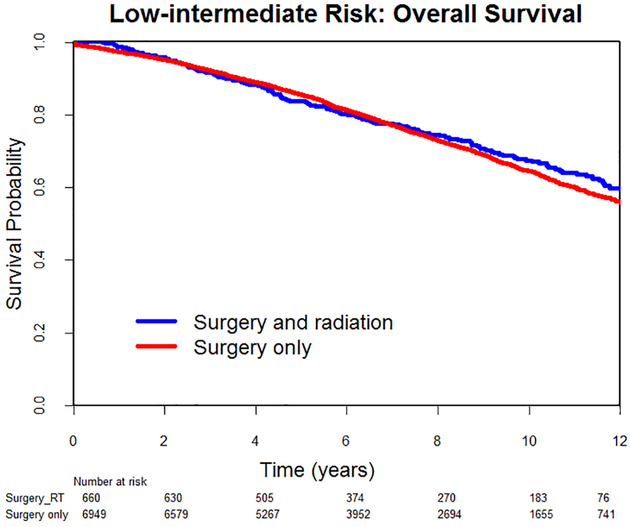
10,842 patients met inclusion criteria. In the LIR group (n = 7609), there was no difference in 10-year overall survival between patients who received radiotherapy and those who did not (67% vs 65%, adjusted HR 0.95, 95% CI 0.81-1.11). In the HIR group (n = 3233), patients who underwent radiotherapy had a significant increase in survival (60% vs 47%, aHR 0.75, 95% CI 0.67-0.85). Radiotherapy was associated with increased costs compared to surgery alone ($26,585 vs $16,712, p < .001). Costs for patients receiving VBT, EBRT, and concurrent VBT/EBRT were $24,044, $27,512, and $31,564, respectively (p < .001). Radiotherapy was associated with an increased risk of gastrointestinal (7 vs 4%), genitourinary (2 vs 1%), and hematologic (16 vs 12%) complications (p < .001).
Radiotherapy was associated with improved survival in women with HIR, but not in LIR. It also had increased costs and a higher morbidity risk. Consideration of observation without radiotherapy in LIR may be reasonable.
评估接受和不接受辅助放疗的低危(LIR)和高危子宫内膜癌(HIR)女性的治疗模式、结局和成本。
从 SEER-Medicare 数据库中确定了 2000 年至 2011 年期间接受手术治疗的所有 I 期子宫内膜样子宫内膜癌患者。LIR 定义为 G1-2 肿瘤,肌层浸润<50%或 G3 无浸润。HIR 定义为 G1-2 肿瘤肌层浸润≥50%或 G3 肿瘤浸润<50%。根据是否接受辅助放疗(阴道近距离放疗[VBT]、外照射放疗[EBRT]或两者)或未放疗对患者进行分类。分析并比较了结果(主要结局为总生存率)。
10842 名患者符合纳入标准。在 LIR 组(n=7609)中,接受放疗与未接受放疗的患者 10 年总生存率无差异(67% vs 65%,调整 HR 0.95,95%CI 0.81-1.11)。在 HIR 组(n=3233)中,接受放疗的患者生存率显著提高(60% vs 47%,aHR 0.75,95%CI 0.67-0.85)。与单独手术相比,放疗相关费用增加(26585 美元 vs 16712 美元,p<.001)。接受 VBT、EBRT 和同时接受 VBT/EBRT 的患者费用分别为 24044 美元、27512 美元和 31564 美元(p<.001)。放疗相关的胃肠道(7% vs 4%)、泌尿生殖系统(2% vs 1%)和血液学(16% vs 12%)并发症风险增加(p<.001)。
在 HIR 女性中,放疗与生存改善相关,但在 LIR 女性中无此相关性。它还增加了成本和更高的发病率风险。在 LIR 中考虑不进行放疗的观察可能是合理的。