From the Department of Medicine F & J. Recanati Autonomic Dysfunction Center, Tel Aviv "Sourasky" Medical Center and Sackler Faculty of Medicine, University of Tel Aviv, Israel (G.J.).
US Department of Veterans Affairs, Tennessee Valley Healthcare System, Nashville (L.D.).
Hypertension. 2019 May;73(5):1087-1096. doi: 10.1161/HYPERTENSIONAHA.118.11803.
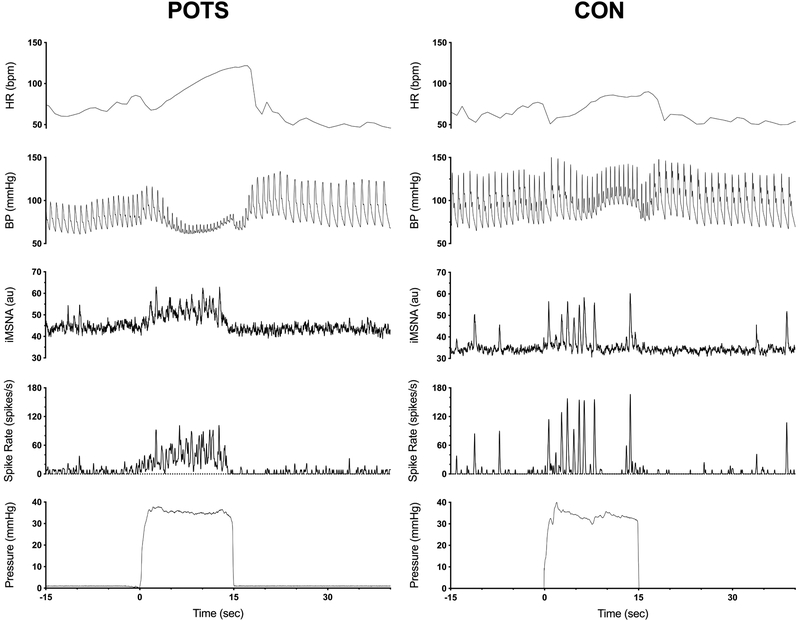
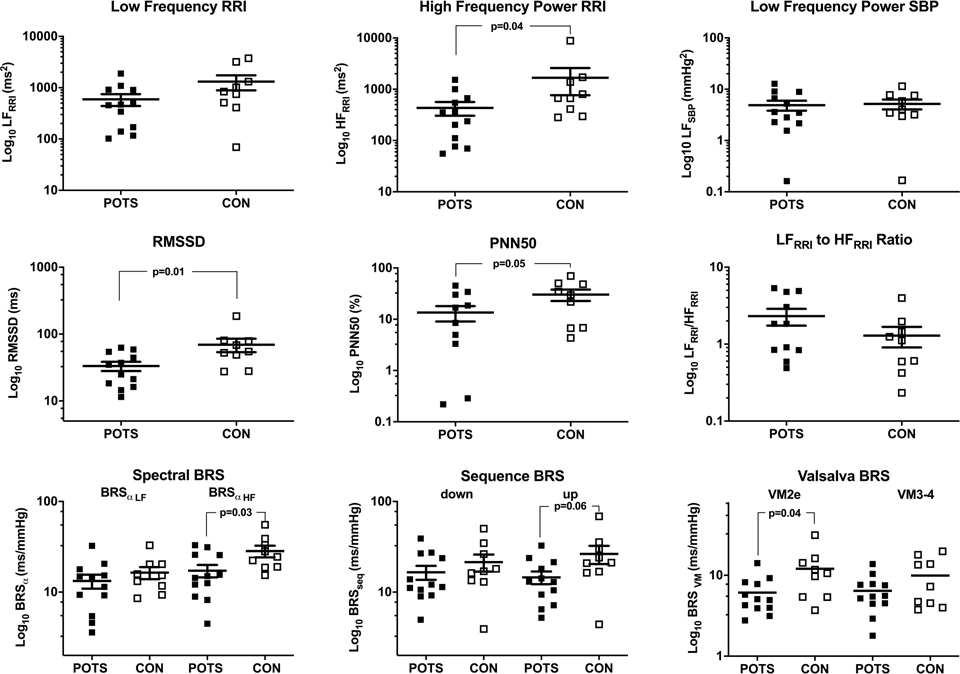
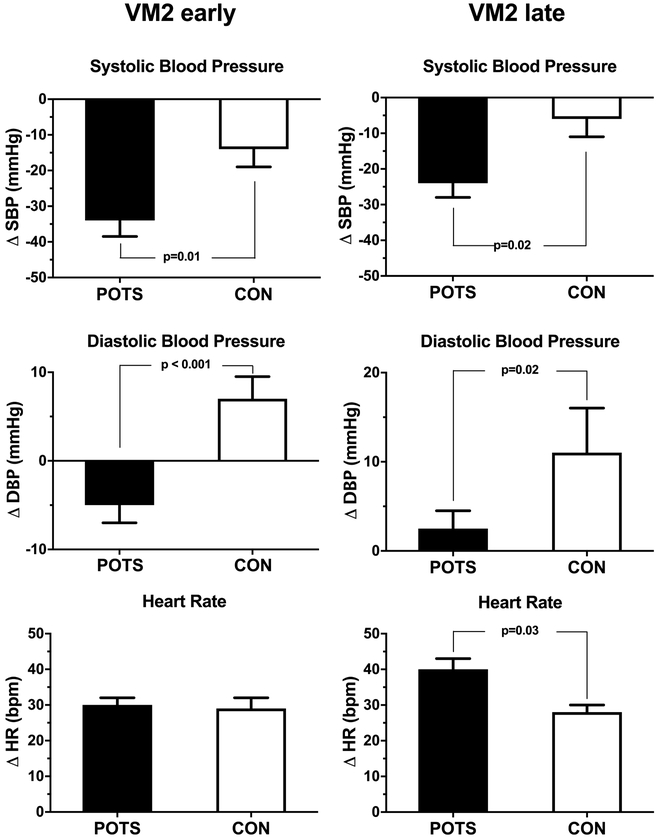
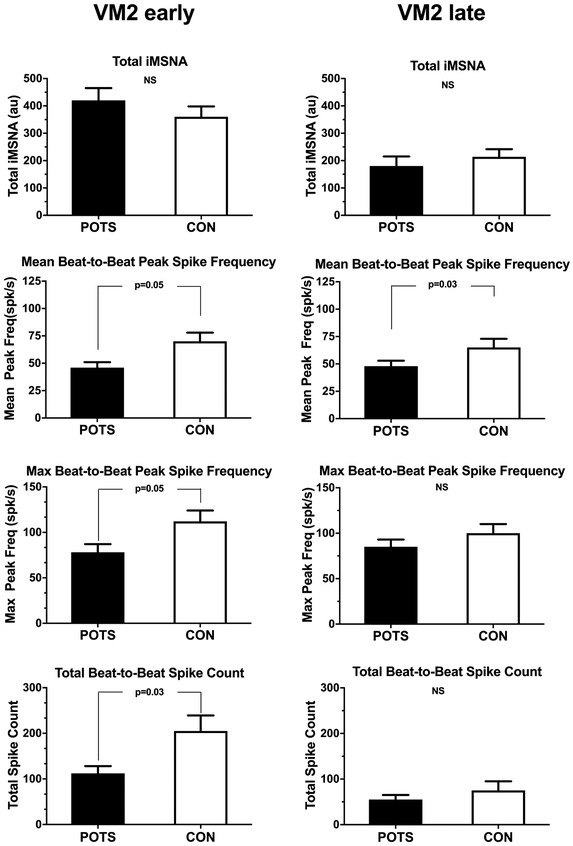
The diagnosis of neuropathic postural tachycardia syndrome (POTS) requires research techniques not available clinically. We hypothesized that these patients will have impaired vagal and sympathetic cardiovascular control that can be characterized with clinical autonomic tests. We included 12 POTS patients with possible neuropathic subtype because of normal plasma norepinephrine and no increase in upright blood pressure. We compared them to 10 healthy subjects. We assessed hemodynamics, heart rate and blood pressure variability, baroreflex sensitivity, raw and integrated muscle sympathetic nerve activity, and blood volume. To understand the vagal/sympathetic control, we dissected the phase 2 of Valsalva maneuver (VM) into early (VM2e) and late (VM2l). POTS' upright heart rate increased 43±3 bpm. Patients had normal plasma volume but reduced red blood cell volume (1.29 L versus predicted normal values 1.58 L; P=0.02). Vagal indices of heart rate variability, HF (430±130 versus 1680±900; P=0.04), PNN50, and root mean squared of successive differences were lower in POTS. Patients showed a decrease in vagal baroreflex sensitivity (VM2e; P=0.04). In POTS, integrated muscle sympathetic nerve activity was lower at rest (12±1.5 versus 20±2 burst/min; P=0.004) and raw muscle sympathetic nerve activity spike analysis showed blunted responses during VM2e, despite a greater drop in systolic blood pressure (34±5 in POTS and 14±6 mm Hg in controls; P=0.01). This cohort of POTS patients enriched for possible neuropathic subtype had lower resting muscle sympathetic nerve activity, impaired vagal cardiac control, and exaggerated drop in blood pressure in response to VM and a delay in the sympathetic cardiovascular responsiveness during hypotensive challenge.
神经病变性体位性心动过速综合征(POTS)的诊断需要使用临床不可用的研究技术。我们假设这些患者会出现迷走神经和交感心血管控制受损的情况,可以通过临床自主神经测试来描述。我们纳入了 12 名可能患有神经病变型 POTS 的患者,因为他们的血浆去甲肾上腺素正常且直立血压没有升高。我们将他们与 10 名健康受试者进行了比较。我们评估了血流动力学、心率和血压变异性、压力感受反射敏感性、原始和整合的肌肉交感神经活动以及血容量。为了了解迷走神经/交感神经的控制,我们将瓦尔萨尔瓦动作(VM)的第 2 期分为早期(VM2e)和晚期(VM2l)。POTS 的直立心率增加了 43±3 次/分。患者的血浆容量正常,但红细胞容量减少(1.29 L 比预测的正常值 1.58 L;P=0.02)。POTS 的心率变异性、HF(430±130 比 1680±900;P=0.04)、PNN50 和均方根连续差异的迷走神经指数较低。患者的迷走神经压力感受反射敏感性降低(VM2e;P=0.04)。在 POTS 中,静息时整合的肌肉交感神经活动较低(12±1.5 比 20±2 爆发/分钟;P=0.004),并且在 VM2e 期间,原始肌肉交感神经活动的尖峰分析显示反应迟钝,尽管收缩压下降更大(34±5 在 POTS 和 14±6 mmHg 在对照组;P=0.01)。这组可能患有神经病变型 POTS 的患者静息时的肌肉交感神经活动较低,迷走神经心脏控制受损,对 VM 的血压下降反应过度,并且在低血压挑战期间交感心血管反应延迟。