Ahmed Haroon, Farewell Daniel, Francis Nick A, Paranjothy Shantini, Butler Christopher C
Division of Population Medicine, Cardiff University School of Medicine, Neuadd Meirionnydd, Heath Park, United Kingdom.
Nuffield Department of Primary Care Health Sciences, University of Oxford, Radcliffe Primary Care Building, Radcliffe Observatory Quarter, United Kingdom.
Open Forum Infect Dis. 2019 Jan 18;6(3):ofz039. doi: 10.1093/ofid/ofz039. eCollection 2019 Mar.
Nitrofurantoin is widely recommended for empirical treatment of urinary tract infection (UTI), but primary care clinicians may prescribe alternative antibiotics to improve prognosis in older, sicker patients. We assessed whether prescribing alternative antibiotics was associated with reduced risk of adverse outcomes in older patients.
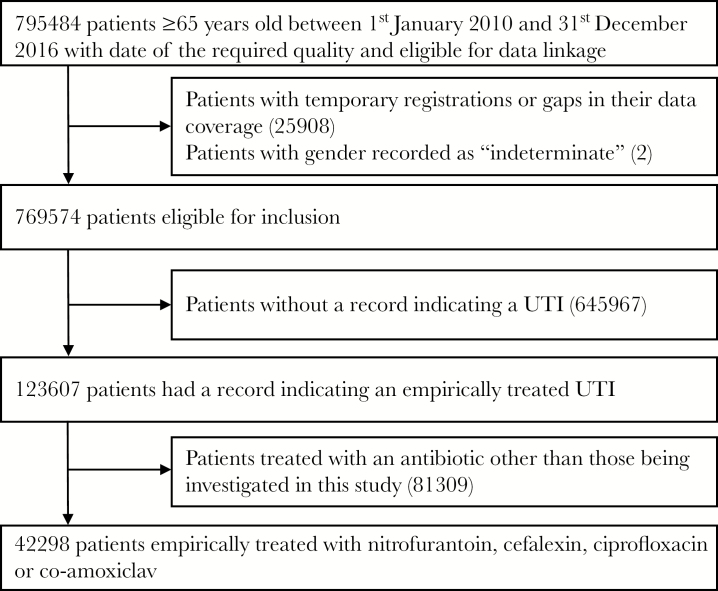
This retrospective cohort study included patients aged ≥65 years empirically treated for a UTI with nitrofurantoin, cefalexin, ciprofloxacin, or co-amoxiclav. We matched patients on their propensity to receive a nitrofurantoin prescription and used mixed-effects logistic regression to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for reconsultation and represcription (proxy for treatment failure), hospitalization for UTI, sepsis, or acute kidney injury, and death.
We identified 42 298 patients aged ≥65 years prescribed empirical nitrofurantoin, cefalexin, ciprofloxacin, or co-amoxiclav for a UTI. Compared with nitrofurantoin, patients prescribed cefalexin, ciprofloxacin, or co-amoxiclav had lower odds of reconsultation and represcription (OR for cefalexin = 0.85, 95% CI = 0.75-0.98; OR for ciprofloxacin = 0.48, 95% CI = 0.38-0.61, OR for co-amoxiclav = 0.77, 95% CI = 0.64-0.93). Patients prescribed cefalexin or ciprofloxacin had greater odds of hospitalization for sepsis (OR for cefalexin = 1.89, 95% CI = 1.03-3.47; OR for ciprofloxacin = 3.21, 95% CI = 1.59-6.50), and patients prescribed cefalexin had greater odds of death (OR = 1.44, 95% CI = 1.12-1.85).
Compared with nitrofurantoin, prescribing of alternative antibiotics for UTI in older people may be associated with lower rates of treatment failure but was not associated with reduced risk of UTI-related hospitalization or death.
呋喃妥因被广泛推荐用于尿路感染(UTI)的经验性治疗,但基层医疗临床医生可能会开具其他抗生素以改善老年、病情较重患者的预后。我们评估了开具其他抗生素是否与降低老年患者不良结局的风险相关。
这项回顾性队列研究纳入了年龄≥65岁、接受呋喃妥因、头孢氨苄、环丙沙星或阿莫西林克拉维酸经验性治疗UTI的患者。我们根据患者接受呋喃妥因处方的倾向进行匹配,并使用混合效应逻辑回归来估计再次咨询和重新开处方(治疗失败的替代指标)、因UTI住院、败血症或急性肾损伤以及死亡的比值比(OR)和95%置信区间(CI)。
我们确定了42298名年龄≥65岁、因UTI开具经验性呋喃妥因、头孢氨苄、环丙沙星或阿莫西林克拉维酸的患者。与呋喃妥因相比,开具头孢氨苄、环丙沙星或阿莫西林克拉维酸的患者再次咨询和重新开处方的几率较低(头孢氨苄的OR = 0.85,95%CI = 0.75 - 0.98;环丙沙星的OR = 0.48,95%CI = 0.38 - 0.61,阿莫西林克拉维酸的OR = 0.77,95%CI = 0.64 - 0.93)。开具头孢氨苄或环丙沙星的患者因败血症住院的几率更高(头孢氨苄的OR = 1.89,95%CI = 1.03 - 3.47;环丙沙星的OR = 3.21,95%CI = 1.59 - 6.50),开具头孢氨苄的患者死亡几率更高(OR = 1.44,95%CI = 1.12 - 1.85)。
与呋喃妥因相比,为老年人UTI开具其他抗生素可能与较低的治疗失败率相关,但与UTI相关住院或死亡风险降低无关。