Wellcome Trust Clinical Research Facility, Western General Hospital, Edinburgh, United Kingdom.
Information Services Division, NHS National Services Scotland, Edinburgh, United Kingdom.
PLoS One. 2019 Mar 19;14(3):e0210452. doi: 10.1371/journal.pone.0210452. eCollection 2019.
The long-term risk of stroke or myocardial infarction (MI) in patients with minor neurological symptoms who are not clinically diagnosed with transient ischaemic attack (TIA) or minor stroke is uncertain.
We used data from a rapid access clinic for patients with suspected TIA or minor stroke and follow-up from four overlapping data sources for a diagnosis of ischaemic or haemorrhagic stroke, MI, major haemorrhage and death. We identified patients with and without a clinical diagnosis of TIA or minor stroke. We estimated hazard ratios of stroke, MI, major haemorrhage and death in early and late time periods.
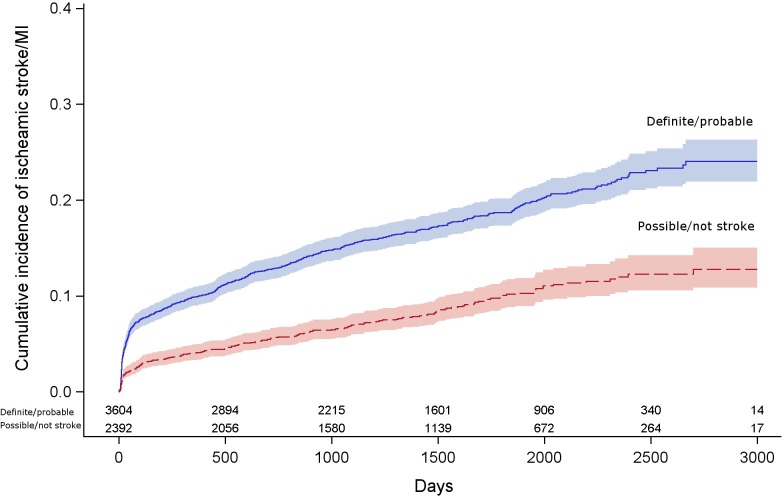
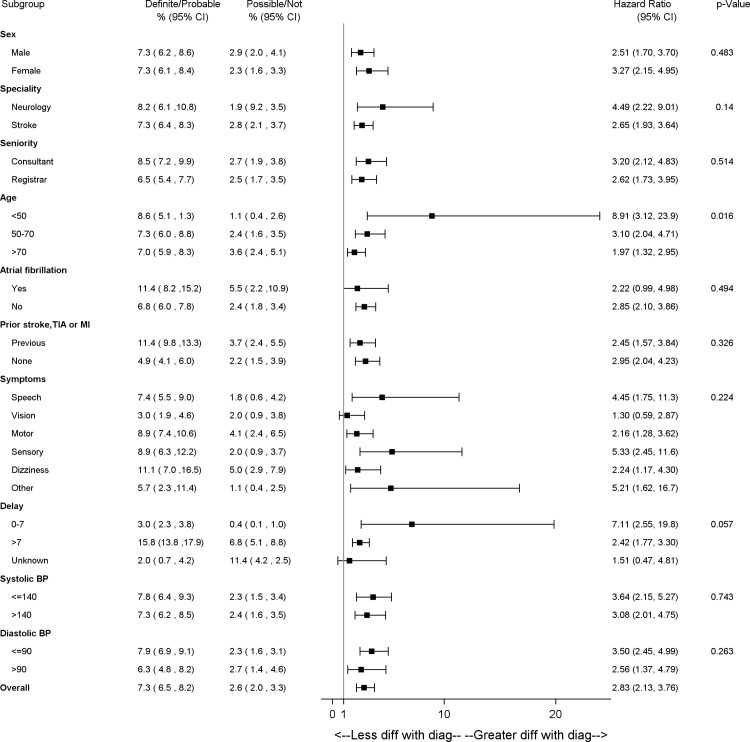
5,997 patients were seen from 2005-2013, who were diagnosed with TIA or minor stroke (n = 3604, 60%) or with other diagnoses (n = 2392, 40%). By 5 years the proportion of patients who had a subsequent ischaemic stroke or MI, in patients with a clinical diagnosis of minor stroke or TIA was 19% [95% confidence interval (CI): 17-20%], and in patients with other diagnoses was 10% (95%CI: 8-15%). Patients with clinical diagnosis of TIA or minor stroke had three times the hazard of stroke or MI compared to patients with other diagnoses [hazard ratio (HR)2.83 95%CI:2.13-3.76, adjusted age and sex] by 90 days post-event; however from 90 days to end of follow up, this difference was attenuated (HR 1.52, 95%CI:1.25-1.86). Older patients and those who had a history of vascular disease had a high risk of stroke or MI, whether or not they were diagnosed with minor stroke or TIA.
Careful attention to vascular risk factors in patients presenting with transient or minor neurological symptoms not thought to be due to stroke or TIA is justified, particularly those who are older or have a history of vascular disease.
患有轻微神经系统症状但未临床诊断为短暂性脑缺血发作(TIA)或小卒中的患者,其卒中或心肌梗死(MI)的长期风险尚不确定。
我们使用疑似 TIA 或小卒中快速就诊患者的数据,并通过四个重叠数据源对缺血性或出血性卒中、MI、大出血和死亡进行诊断。我们确定了有和无 TIA 或小卒中临床诊断的患者。我们估计了早期和晚期时段卒中、MI、大出血和死亡的风险比。
2005 年至 2013 年间共诊治了 5997 例患者,其中诊断为 TIA 或小卒中(n = 3604,60%)或其他诊断(n = 2392,40%)。5 年内,有临床诊断的小卒中或 TIA 的患者中,随后发生缺血性卒中或 MI 的比例为 19%(95%CI:17-20%),而其他诊断的患者中为 10%(95%CI:8-15%)。有 TIA 或小卒中临床诊断的患者发生卒中或 MI 的风险是其他诊断患者的 3 倍(风险比[HR]2.83,95%CI:2.13-3.76,校正年龄和性别),但在事件发生后 90 天至随访结束时,这种差异减弱(HR 1.52,95%CI:1.25-1.86)。老年患者和有血管疾病史的患者,无论是否诊断为小卒中或 TIA,发生卒中或 MI 的风险均较高。
对于出现短暂性或轻微神经系统症状但不认为是由卒中或 TIA 引起的患者,应对血管危险因素进行仔细评估,尤其是那些年龄较大或有血管疾病史的患者。