a Head and Neck Research Group, Research Centre, Akershus University Hospital , Oslo , Norway.
b Institute of Clinical Medicine, Akershus University Hospital, University of Oslo , Nordbyhagen , Norway.
Ann Med. 2019 Mar;51(2):118-127. doi: 10.1080/07853890.2019.1590627. Epub 2019 Apr 6.
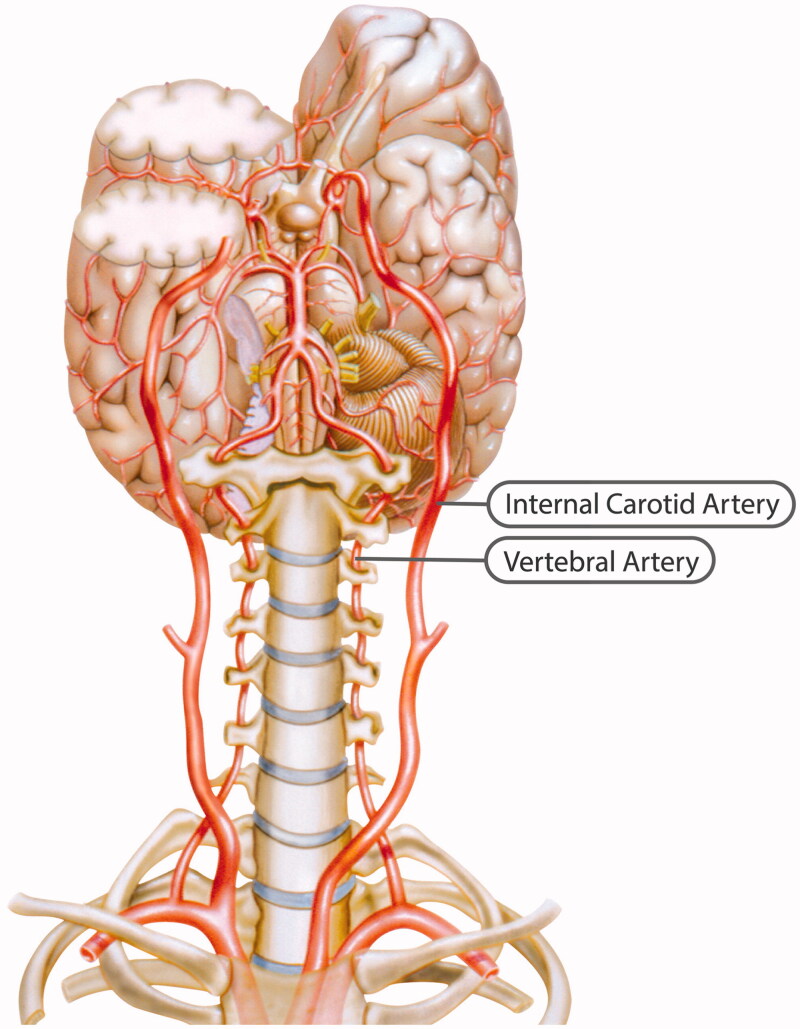
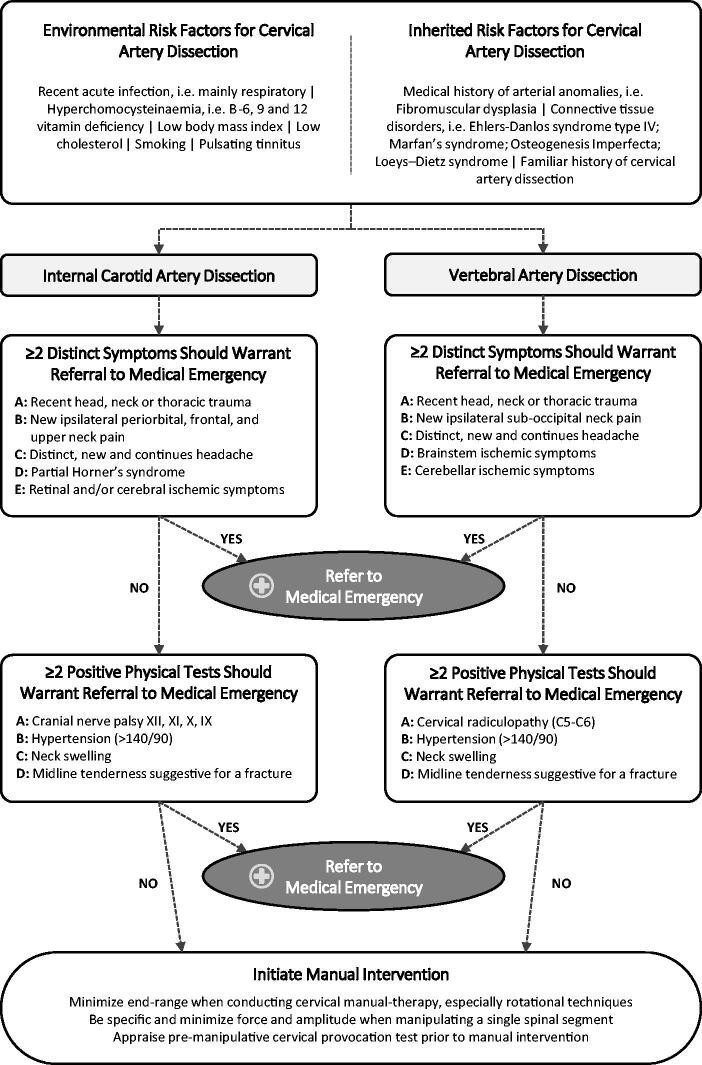
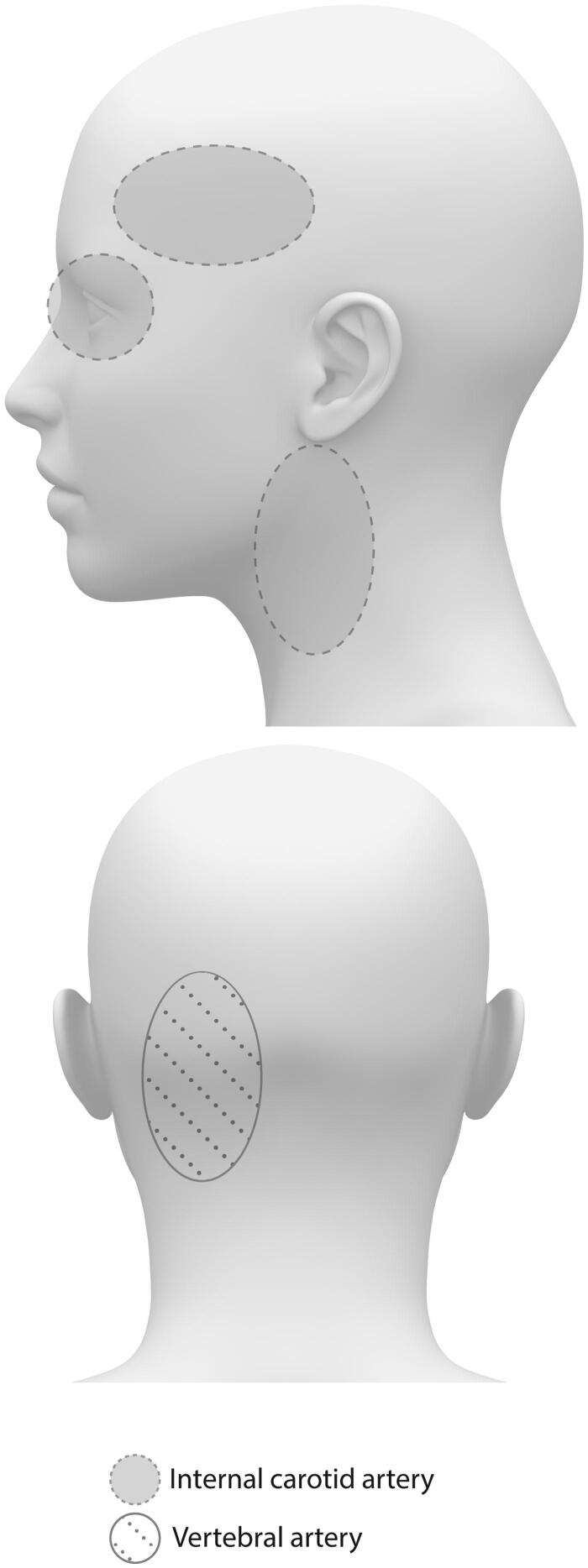
Cervical artery dissection refers to a tear in the internal carotid or the vertebral artery that results in an intramural haematoma and/or an aneurysmal dilatation. Although cervical artery dissection is thought to occur spontaneously, physical trauma to the neck, especially hyperextension and rotation, has been reported as a trigger. Headache and/or neck pain is the most common initial symptom of cervical artery dissection. Other symptoms include Horner's syndrome and lower cranial nerve palsy. Both headache and/or neck pain are common symptoms and leading causes of disability, while cervical artery dissection is rare. Patients often consult their general practitioner for headache and/or neck pain, and because manual-therapy interventions can alleviate headache and/or neck pain, many patients seek manual therapists, such as chiropractors and physiotherapists. Cervical mobilization and manipulation are two interventions that manual therapists use. Both interventions have been suspected of being able to trigger cervical artery dissection as an adverse event. The aim of this review is to provide an updated step-by-step risk-benefit assessment strategy regarding manual therapy and to provide tools for clinicians to exclude cervical artery dissection. Key messages Cervical mobilization and/or manipulation have been suspected to be able to trigger cervical artery dissection (CAD). However, these assumptions are based on case studies which are unable to established direct causality. The concern relates to the chicken and the egg discussion, i.e. whether the CAD symptoms lead the patient to seek cervical manual-therapy or whether the cervical manual-therapy provoked CAD along with the non-CAD presenting complaint. Thus, instead of proving a nearly impossible causality hypothesis, this study provide clinicians with an updated step-by-step risk-benefit assessment strategy tool to (a) facilitate clinicians understanding of CAD, (b) appraise the risk and applicability of cervical manual-therapy, and (c) provide clinicians with adequate tools to better detect and exclude CAD in clinical settings.
颈内动脉夹层是指颈内动脉或椎动脉的内膜撕裂,导致壁内血肿和/或动脉瘤样扩张。尽管颈内动脉夹层被认为是自发性发生的,但颈部的物理创伤,特别是伸展和旋转,已被报道为触发因素。头痛和/或颈痛是颈内动脉夹层最常见的初始症状。其他症状包括霍纳氏综合征和颅神经麻痹。头痛和/或颈痛是常见的症状和导致残疾的主要原因,而颈内动脉夹层则很少见。患者经常因头痛和/或颈痛就诊于全科医生,并且由于手法治疗干预可以缓解头痛和/或颈痛,因此许多患者会寻求手法治疗师,如按摩师和物理治疗师。颈椎活动和手法是手法治疗师使用的两种干预措施。这两种干预措施都被怀疑可能引发颈内动脉夹层作为不良事件。本综述的目的是提供一种关于手法治疗的更新的逐步风险效益评估策略,并为临床医生提供排除颈内动脉夹层的工具。关键信息颈椎活动和/或手法已被怀疑能够引发颈内动脉夹层(CAD)。然而,这些假设基于病例研究,无法确定直接因果关系。关注的问题涉及到鸡和蛋的讨论,即 CAD 症状是否导致患者寻求颈椎手法治疗,还是颈椎手法治疗与非 CAD 主诉一起引发 CAD。因此,本研究不是为了证明几乎不可能的因果关系假设,而是为临床医生提供了一种更新的逐步风险效益评估策略工具,以(a)帮助临床医生了解 CAD,(b)评估颈椎手法治疗的风险和适用性,以及(c)为临床医生提供足够的工具,以便在临床环境中更好地检测和排除 CAD。