Department of Anaesthesiology and Pain Medicine, Severance Hospital, Anaesthesia and Pain Research Institute, Yonsei University College of Medicine, 50-1 Yonsei-ro, Seodaemun-gu, Seoul, 03722, Korea.
Department of Policy Research Affairs, National Health Insurance Service Ilsan Hospital, Goyang, Gyeonggi-do, Korea.
BMC Cancer. 2019 Mar 20;19(1):251. doi: 10.1186/s12885-019-5451-5.
Dexamethasone is widely used in cancer patients despite the concern that perioperative glucocorticoids may potentially cause immunosuppression. However, studies on the influence of dexamethasone on cancer recurrence after curative surgery have produced conflicting results. The goal of our study was to compare postoperative recurrence-free survival and overall survival between patients with breast cancer who received perioperative dexamethasone and those who did not.
The medical records of 2729 patients who underwent breast cancer surgery between November 2005 and December 2010 were reviewed. These patients were followed up until December 2015. The patients were categorised according whether they received a single dose of intravenous dexamethasone perioperatively or not. Cox regression analyses were conducted to evaluate any associations between dexamethasone usage with postoperative recurrence and mortality. Additionally, we performed a sensitivity test with propensity score matching to adjust for selection bias.
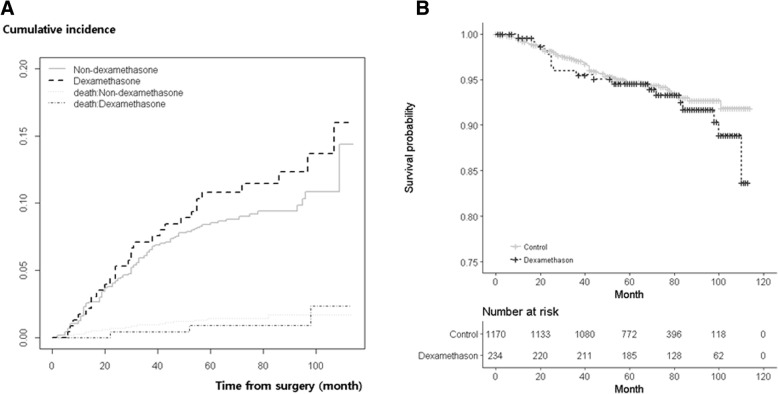
Among the 2628 patients, 236 (8.5%) received perioperative dexamethasone. No increasing risk for recurrence (hazard ratio [HR], 1.442; 95% confidence interval [CI], 0.969-2.145; P = 0.071) or mortality (HR, 1.256; 95% CI, 0.770-2.047; P = 0.361) after breast cancer surgery were identified in patients who received dexamethasone. Similarly, propensity score matching did not show significant associations in postoperative recurrence (HR, 1.389; 95% CI, 0.904-2.132; P = 0.133) or mortality (HR, 1.506; 95% CI, 0.886-2.561; P = 0.130) in patients who received dexamethasone.
We found that a perioperative single dose of dexamethasone is not associated with increased recurrence or mortality after curative surgery in breast cancer patients.
尽管围手术期糖皮质激素可能会导致免疫抑制,但地塞米松仍广泛用于癌症患者。然而,关于地塞米松对根治性手术后癌症复发的影响的研究结果却相互矛盾。我们的研究目的是比较接受和不接受围手术期地塞米松治疗的乳腺癌患者的无复发生存和总生存情况。
回顾了 2005 年 11 月至 2010 年 12 月期间接受乳腺癌手术的 2729 例患者的病历。这些患者随访至 2015 年 12 月。根据患者是否接受围手术期单次静脉注射地塞米松将其分为两组。采用 Cox 回归分析评估地塞米松使用与术后复发和死亡之间的任何关联。此外,我们还进行了倾向评分匹配的敏感性测试,以调整选择偏倚。
在 2628 例患者中,有 236 例(8.5%)接受了围手术期地塞米松治疗。与未接受地塞米松治疗的患者相比,接受地塞米松治疗的患者乳腺癌手术后复发的风险没有增加(风险比 [HR],1.442;95%置信区间 [CI],0.969-2.145;P=0.071)或死亡风险(HR,1.256;95%CI,0.770-2.047;P=0.361)。同样,倾向评分匹配也未显示接受地塞米松治疗的患者术后复发(HR,1.389;95%CI,0.904-2.132;P=0.133)或死亡(HR,1.506;95%CI,0.886-2.561;P=0.130)的风险存在显著相关性。
我们发现,乳腺癌患者围手术期单次剂量地塞米松的使用与根治性手术后的复发或死亡无关。