Kato K, Ezoe K, Yabuuchi A, Fukuda J, Kuroda T, Ueno S, Fujita H, Kobayashi T
Kato Ladies Clinic, Tokyo 160-0023, Japan.
Hum Reprod Open. 2018 Apr 25;2018(3):hoy006. doi: 10.1093/hropen/hoy006. eCollection 2018.
Are there any differences in live birth rates (LBR) following fresh blastocyst transfer in natural or clomiphene-stimulated cycles, or after elective blastocyst freezing in clomiphene-stimulated cycles followed by thawing and transfer at different time-points?
Clomiphene citrate (CC) administration adversely affected the LBR after single fresh blastocyst transfer (SBT) in CC cycles compared with that in natural cycles, while this adverse effect of CC is not present when a single vitrified-warmed blastocyst transfer (SVBT) is performed in subsequent natural ovulatory cycles, regardless of the duration between CC administration and the day of SVBT.
CC affects uterine receptivity associated with a thinning of the uterine endometrium through an antioestrogenic effect. However, the duration that this adverse effect of CC on uterine endometrium persists after initial use is still unknown.
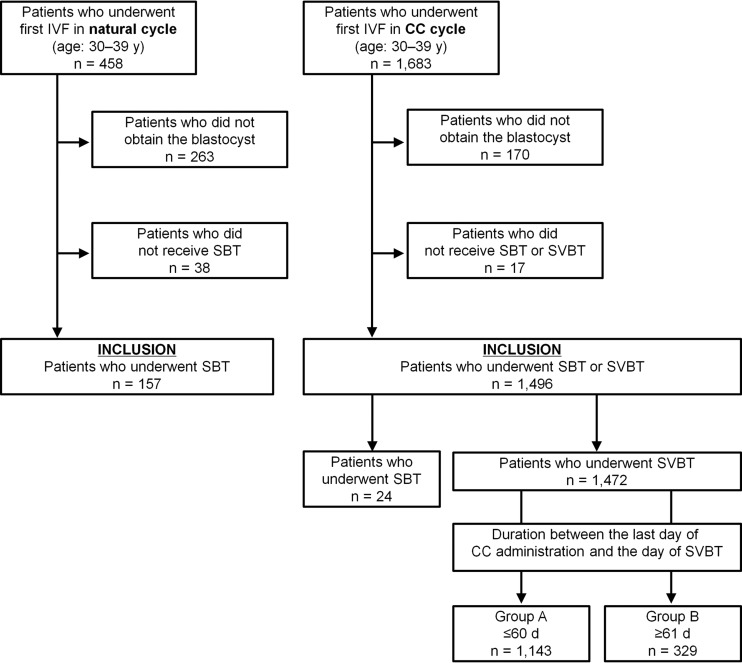
A retrospective cohort study of 157 natural cycle IVFs followed by SBT and 1496 minimal ovarian stimulation with CC IVF cycles followed by SBT ( = 24) or SVBT ( = 1472) from January 2010 to December 2014 was conducted. SVBT cycles were classified into two groups according to the period between the last day of CC administration and the day of SVBT (A: ≤60 d and B: ≥61 d). All groups were then compared based on pregnancy outcomes (natural-SBT group: = 157, CC-SBT group: = 24, SVBT-A: = 1143, SVBT-B: = 329).
PARTICIPANTS/MATERIALS SETTING METHODS: Women were aged 30-39 years at oocyte retrieval. In SVBT cycles, blastocysts were vitrified and warmed using a Cryotop safety kit. SVBT was performed in subsequent natural ovulatory cycles. The main outcomes were LBR and neonatal outcome, and both were compared among the groups.
The LBR in the CC-SBT group (29.2%, 7/24) was significantly lower compared with the natural-SBT (56.1%, 88/157) ( = 0.01) and SVBT-A (50.0%, 572/1143) ( = 0.04), but not SVBT-B (47.4%, 156/329), groups. Furthermore, multivariate logistic regression analysis revealed that the LBR was comparable among the natural-SBT and SVBT groups, but was significantly lower in the CC-SBT group (adjusted odds ratio: 0.324, 95% CI: 0.119-0.800, = 0.01). No significant differences among all groups were observed for gestational age ( = 0.19), birthweight ( = 0.41) and incidence of malformation ( = 0.53).
In this study we analysed a biased sample, based on clinical judgement regarding endometrial thickness, and the study was limited by its retrospective nature. The low statistical power caused by the group size disparity was also a limitation, especially in the CC-SBT group. Although the outcome showing inferiority of CC-SBT compared to natural-SBT is consistent with general findings in the literature, further large-scale clinical studies, ideally RCTs, are necessary to validate our results and clarify the prolonged effect of CC in SVBT cycles on pregnancy and neonatal outcomes.
Our observation suggests that CC administered in minimal ovarian stimulation cycles affects adversely the pregnancy outcomes when SBT is performed. Therefore, for a CC-based minimal stimulation IVF cycle, we suggest that frozen embryo transfer should be performed in a subsequent natural ovulatory cycle to avoid the possibility of implantation failure associated with CC administration.
STUDY FUNDING/COMPETING INTERESTS: The authors have no conflicts of interest to declare. No external funding was either sought or obtained.
在自然周期或克罗米芬刺激周期中进行新鲜囊胚移植后,活产率(LBR)是否存在差异?或者在克罗米芬刺激周期中进行选择性囊胚冷冻,随后在不同时间点解冻并移植后,活产率是否存在差异?
与自然周期相比,在克罗米芬周期中单次新鲜囊胚移植(SBT)后,服用枸橼酸克罗米芬(CC)对活产率有不利影响;而在随后的自然排卵周期中进行单次玻璃化冷冻囊胚移植(SVBT)时,无论CC给药与SVBT日之间的间隔时间长短,CC的这种不利影响均不存在。
CC通过抗雌激素作用影响与子宫内膜变薄相关的子宫容受性。然而,CC对子宫内膜的这种不利影响在初次使用后持续的时间仍不清楚。
研究设计、规模、持续时间:对2010年1月至2014年12月期间157例自然周期体外受精后进行SBT以及1496例接受CC最小剂量卵巢刺激的体外受精周期后进行SBT(n = 24)或SVBT(n = 1472)的患者进行了一项回顾性队列研究。SVBT周期根据CC给药最后一天与SVBT日之间的时间间隔分为两组(A组:≤60天;B组:≥61天)。然后根据妊娠结局对所有组进行比较(自然周期-SBT组:n = 157,CC-SBT组:n = 24,SVBT-A组:n = 1143,SVBT-B组:n = 329)。
参与者/材料、环境、方法:取卵时女性年龄为30 - 39岁。在SVBT周期中,使用Cryotop安全试剂盒对囊胚进行玻璃化冷冻和解冻。在随后的自然排卵周期中进行SVBT。主要结局为活产率和新生儿结局,并在各组之间进行比较。
CC-SBT组的活产率(29.2%,7/24)显著低于自然周期-SBT组(56.1%,88/157)(P = 0.01)和SVBT-A组(50.0%,572/1143)(P = 0.04),但与SVBT-B组(47.4%,156/329)相比无显著差异。此外,多因素逻辑回归分析显示,自然周期-SBT组和SVBT组的活产率相当,但CC-SBT组显著更低(调整后的优势比:0.324,95%可信区间:0.119 - 0.800,P = 0.01)。在胎龄(P = 0.19)、出生体重(P = 0.41)和畸形发生率(P = 0.53)方面,各组之间未观察到显著差异。
局限性、谨慎的原因:在本研究中,我们基于对子宫内膜厚度的临床判断分析了一个有偏样本,且该研究受其回顾性性质所限。组间样本量差异导致的低统计效能也是一个局限性,尤其是在CC-SBT组。尽管CC-SBT组与自然周期-SBT组相比活产率较低的结果与文献中的一般发现一致,但仍需要进一步的大规模临床研究,理想情况下是随机对照试验,以验证我们的结果并阐明CC在SVBT周期中对妊娠和新生儿结局的长期影响。
我们的观察表明,在最小剂量卵巢刺激周期中使用CC进行SBT时会对妊娠结局产生不利影响。因此,对于基于CC的最小刺激体外受精周期,我们建议在随后的自然排卵周期中进行冷冻胚胎移植,以避免与CC给药相关的植入失败的可能性。
研究资金/利益冲突:作者声明无利益冲突。未寻求或获得外部资金。