Franasiak Jason M, Forman Eric J, Patounakis George, Hong Kathleen H, Werner Marie D, Upham Kathleen M, Treff Nathan R, Scott Richard T
Division of Reproductive Endocrinology, Department of Obstetrics and Gynecology, Thomas Jefferson University, Philadelphia, PA, USA.
Reproductive Medicine Associates of New Jersey, Basking Ridge, NJ, USA.
Hum Reprod Open. 2018 Dec 20;2018(4):hoy022. doi: 10.1093/hropen/hoy022. eCollection 2018.
Do embryos with delayed blastulation have inferior reproductive potential or poorer outcomes due in part to embryo and endometrial synchrony?
Diminished outcomes in embryos with delayed blastulation undergoing fresh embryo transfer (ET) may be attributed to a loss of embryonic-endometrial synchrony.
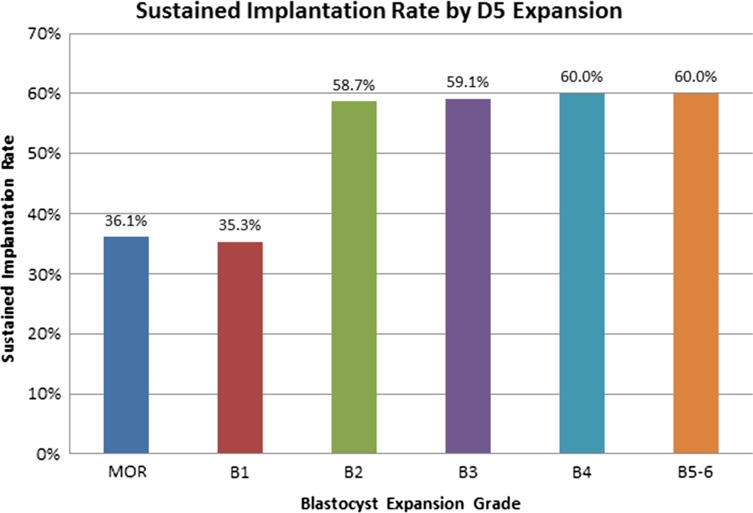
Embryos that blastulate slowly have lower sustained implantation rates (SIR) than those which blastulate normally on Day 5 (D5). Traditionally this has been attributed to reduced embryo quality; however, dyssynchrony with the endometrium is also a possibility and has not been fully described. This convenient cohort composed of groups that resulted from a practice wide change in laboratory protocol allows for evaluation of embryo and endometrial synchrony as it related to blastocyst expansion.
A retrospective cohort analysis was carried out from January 2009 to February 2013. Three cohorts were identified: D5 ET, D6 ET and frozen ET that comprised 822 patients, 763 patients and 718 patients, respectively. Each of these cohorts had slowly blastulating and normally blastulating embryos identified.
PARTICIPANTS/MATERIALS SETTING METHODS: The study setting was academic affiliated private practice. All first fresh or cryopreserved ETs from 2010 to 2013 were studied. Non-biopsied embryos were classified into two groups on D5: slowly blastulating (Morula-Gardner 1) or normally blastulating (Gardner 2-6). Only single ETs or transfer of two embryos within the same classification group were included. Outcomes were compared between classification groups in embryos undergoing transfer on D5, D6, or after cryopreservation. This assesses the impact of transfer timing in fresh cycles as well as isolating a pure embryonic factor in frozen ET cycles. Sustained implantation was defined as heart beat detection at discharge sonogram at 8 weeks gestation. SIR was defined as the number of embryos transferred meeting criteria for sustained implantation divided by the total number of embryos transferred.
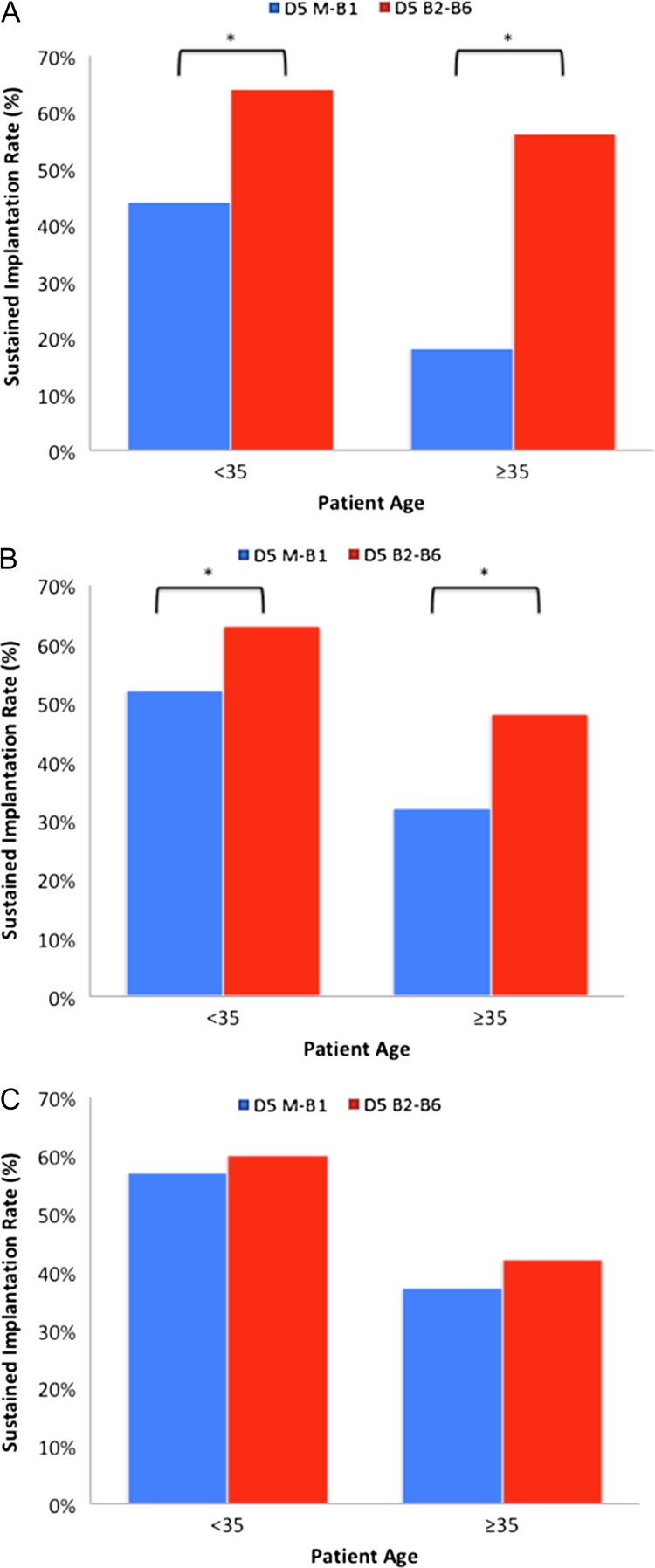
In total, 3391 embryos were transferred to 1966 patients. On D5, SIRs were significantly lower with slowly blastulating embryos (44% versus 64% in women <35 years of age ( < 0.001) and 18% versus 56% in women ≥35 years of age ( < 0.001)). Fresh D6 ETs also had significantly lower SIRs for embryos that were slowly blastulating on D5 (52% versus 63% in <35 years of age ( < 0.05) and 32% versus 48% in ≥35 years of age ( < 0.005)) despite continued development to full blastocysts and being morphologically equivalent at the time of ET, suggesting dyssynchrony. However, when slowly blastulating embryos underwent vitrification and then ET, they had SIRs which were equivalent to their normally blastulating counterparts (57% versus 60% in <35 years of age ( = 0.5) and 37% versus 42% in ≥35 years of age ( = 0.3)). An intraclass correlation and a generalized estimating equation corrected for patient age was performed which confirmed these findings. The normalization in cryopreserved ETs indicates that dyssynchrony may be a major adverse factor limiting outcomes with late blastulating embryos in fresh cycles.
This is a retrospective study comprising cohorts from a convenient sample chosen due to a uniform change in embryology laboratory protocol regarding ET day, however, this was done independent of the management of embryo and endometrial synchrony. Although strict ultrasound and serum progesterone criteria were utilized to make endometrial receptivity uniform, pathologic states of pre-receptive and post-receptive endometrium cannot be ruled out.
The data surrounding embryo and endometrial synchrony should be considered in patients undergoing IVF and attention to the variations in blastulation rates can be applied to any patient undergoing extended embryo culture.
STUDY FUNDING/COMPETING INTERESTS: None.
囊胚形成延迟的胚胎是否具有较低的生殖潜能或较差的结局,部分原因是否在于胚胎与子宫内膜不同步?
新鲜胚胎移植(ET)中囊胚形成延迟的胚胎结局较差,可能归因于胚胎 - 子宫内膜不同步。
囊胚形成缓慢的胚胎与在第5天(D5)正常形成囊胚的胚胎相比,持续着床率(SIR)较低。传统上,这归因于胚胎质量下降;然而,与子宫内膜不同步也是一种可能性,且尚未得到充分描述。这个便利的队列由实验室方案在整个实践范围内改变而形成的几组组成,这使得可以评估与囊胚扩张相关的胚胎和子宫内膜同步性。
研究设计、规模、持续时间:2009年1月至2013年2月进行了一项回顾性队列分析。确定了三个队列:D5 ET、D6 ET和冷冻ET,分别包括822例患者、763例患者和718例患者。这些队列中的每一个都识别出了囊胚形成缓慢和正常形成囊胚的胚胎。
参与者/材料、设置、方法:研究设置为学术附属私人诊所。研究了2010年至2013年所有首次新鲜或冷冻保存的ET。未活检的胚胎在D5分为两组:囊胚形成缓慢(桑椹胚 - 加德纳1级)或正常形成囊胚(加德纳2 - 6级)。仅包括同一分类组内的单胚胎移植或双胚胎移植。比较了在D5、D6进行移植的胚胎或冷冻保存后不同分类组之间的结局。这评估了新鲜周期中移植时间的影响,以及在冷冻ET周期中分离出纯粹的胚胎因素。持续着床定义为妊娠8周时出院超声检查检测到心跳。SIR定义为达到持续着床标准的移植胚胎数除以移植胚胎总数。
总共将3391个胚胎移植给1966例患者。在D5,囊胚形成缓慢的胚胎SIR显著较低(年龄<35岁的女性中分别为44%对64%(P<0.001),年龄≥35岁的女性中分别为18%对56%(P<0.001))。对于在D5囊胚形成缓慢的胚胎,新鲜D6 ET的SIR也显著较低(年龄<35岁的女性中分别为52%对63%(P<0.05),年龄≥35岁的女性中分别为32%对48%(P<0.005)),尽管这些胚胎持续发育至完全囊胚且在ET时形态学上相当,提示不同步。然而,当囊胚形成缓慢的胚胎进行玻璃化然后ET时,它们的SIR与正常形成囊胚的对应胚胎相当(年龄<35岁的女性中分别为57%对6%(P = 0.5),年龄≥35岁的女性中分别为37%对42%(P = 0.3))。进行了组内相关分析和校正患者年龄后的广义估计方程分析,证实了这些发现。冷冻ET中的标准化表明,不同步可能是限制新鲜周期中囊胚形成延迟胚胎结局的主要不利因素。
局限性、谨慎的原因:这是一项回顾性研究,队列来自因胚胎学实验室关于ET日的统一变化而选择的便利样本,然而,这是在独立于胚胎和子宫内膜同步管理的情况下进行的。尽管采用了严格的超声和血清孕酮标准使子宫内膜容受性均匀,但不能排除子宫内膜容受前和容受后的病理状态。
在接受体外受精的患者中应考虑围绕胚胎和子宫内膜同步性的数据,并且对囊胚形成率变化的关注可应用于任何接受延长胚胎培养的患者。
研究资金/利益冲突:无。