Department of Physical Therapy, College of Applied Health Sciences, University of Illinois at Chicago, 1919, W Taylor St, (M/C 898), Chicago, IL, 60612, USA.
J Neuroeng Rehabil. 2019 Mar 22;16(1):43. doi: 10.1186/s12984-019-0510-3.
A single-session of slip-perturbation training has shown to induce long-term fall risk reduction in older adults. Considering the spectrum of motor impairments and deficits in reactive balance after a cortical stroke, we aimed to determine if chronic stroke survivors could acquire and retain reactive adaptations to large slip-like perturbations and if these adaptations were dependent on severity of motor impairment.
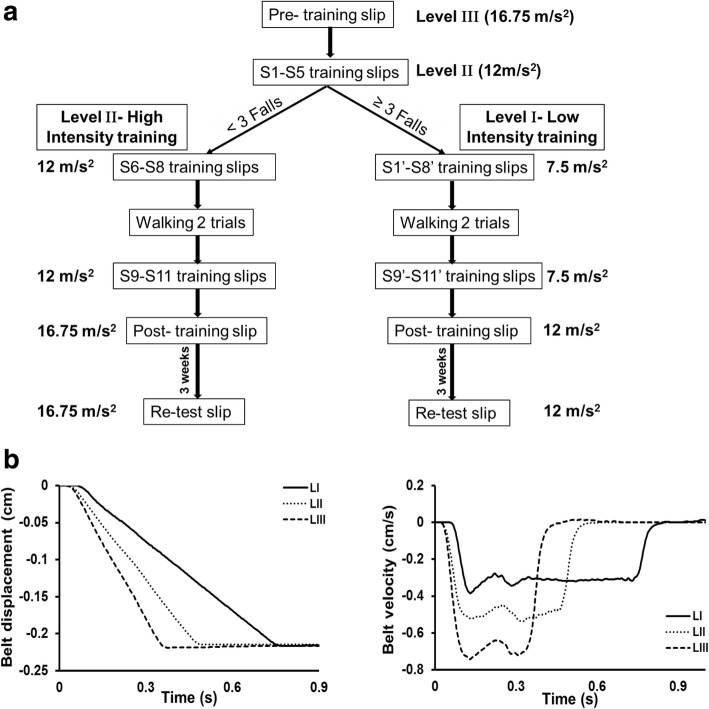
Twenty-six chronic stroke participants were categorized into high and low-functioning groups based on their Chedoke-McMaster-Assessment scores. All participants received a pre-training, slip-like stance perturbation at level-III (highest intensity/acceleration) followed by 11 perturbations at a lower intensity (level-II). If in early phase, participants experienced > 3/5 falls, they were trained at a still lower intensity (level-I). Post-training, immediate scaling and short-term retention at 3 weeks post-training was examined. Perturbation outcome and post-slip center-of-mass (COM) stability was analyzed.
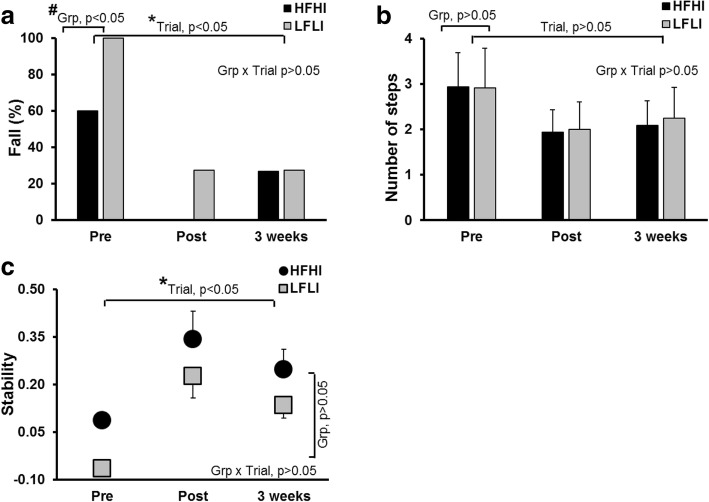
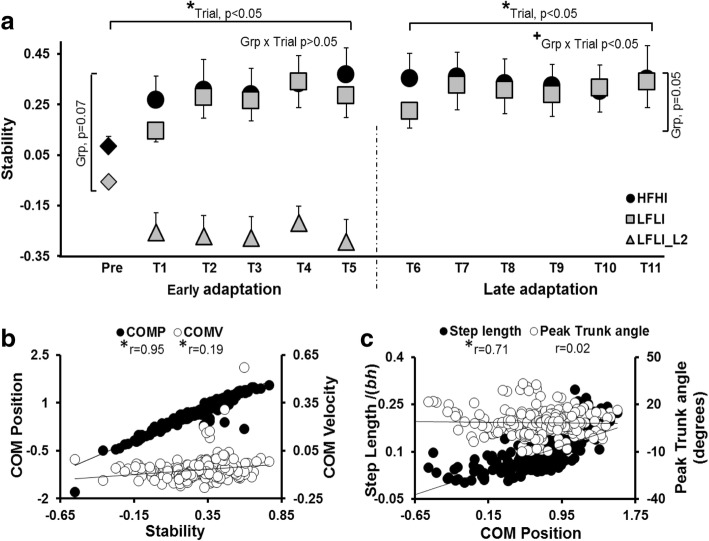
On the pre-training trial, 60% of high and 100% of low-functioning participants fell. High-functioning group tolerated and adapted at training-intensity level-II but low-functioning group were trained at level-I (all had > 3 falls on level-II). At respective training intensities, both groups significantly lowered fall incidence from 1st through 11th trials, with improved post-slip stability and anterior shift in COM position, resulting from increased compensatory step length. Both groups demonstrated immediate scaling and short-term retention of the acquired stability control.
Chronic stroke survivors are able to acquire and retain adaptive reactive balance skills to reduce fall risk. Although similar adaptation was demonstrated by both groups, the low-functioning group might require greater dosage with gradual increment in training intensity.
单次滑动扰动训练已显示可降低老年人的长期跌倒风险。考虑到皮质性中风后运动障碍和反应性平衡缺陷的范围,我们旨在确定慢性中风幸存者是否可以获得并保持对大滑动样扰动的反应性适应,以及这些适应是否取决于运动障碍的严重程度。
根据 Chedoke-McMaster 评估评分,将 26 名慢性中风参与者分为高功能和低功能组。所有参与者均接受预训练,在 III 级(最高强度/加速度)进行类似滑动的站立姿势扰动,然后在较低强度(II 级)进行 11 次扰动。如果在早期阶段,参与者经历了 > 3/5 的跌倒,则在更低的强度(I 级)进行训练。进行训练后,立即进行测试,在训练后 3 周进行短期保留测试。分析了扰动结果和滑动后质心(COM)稳定性。
在预训练试验中,高功能组有 60%的参与者和低功能组有 100%的参与者跌倒。高功能组在训练强度 II 级时可以耐受和适应,但低功能组在 I 级时进行训练(所有在 II 级时都有 > 3 次跌倒)。在各自的训练强度下,两组在第 1 次到第 11 次试验中均显著降低了跌倒发生率,滑动后稳定性提高,COM 位置向前移动,这是由于补偿性步长增加所致。两组均表现出即时的适应能力,并保留了获得的稳定性控制。
慢性中风幸存者能够获得并保持适应性反应性平衡技能,以降低跌倒风险。尽管两组均表现出类似的适应,但低功能组可能需要更高的剂量,并逐渐增加训练强度。