Department of Anesthesiology, Heidelberg University Hospital, Heidelberg, Germany.
Front Immunol. 2019 Mar 12;10:432. doi: 10.3389/fimmu.2019.00432. eCollection 2019.
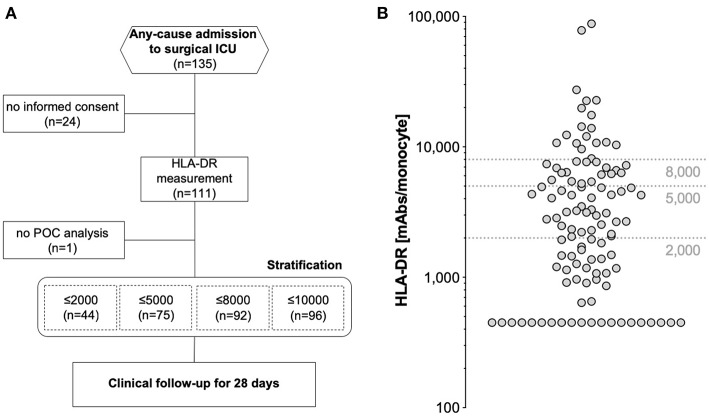
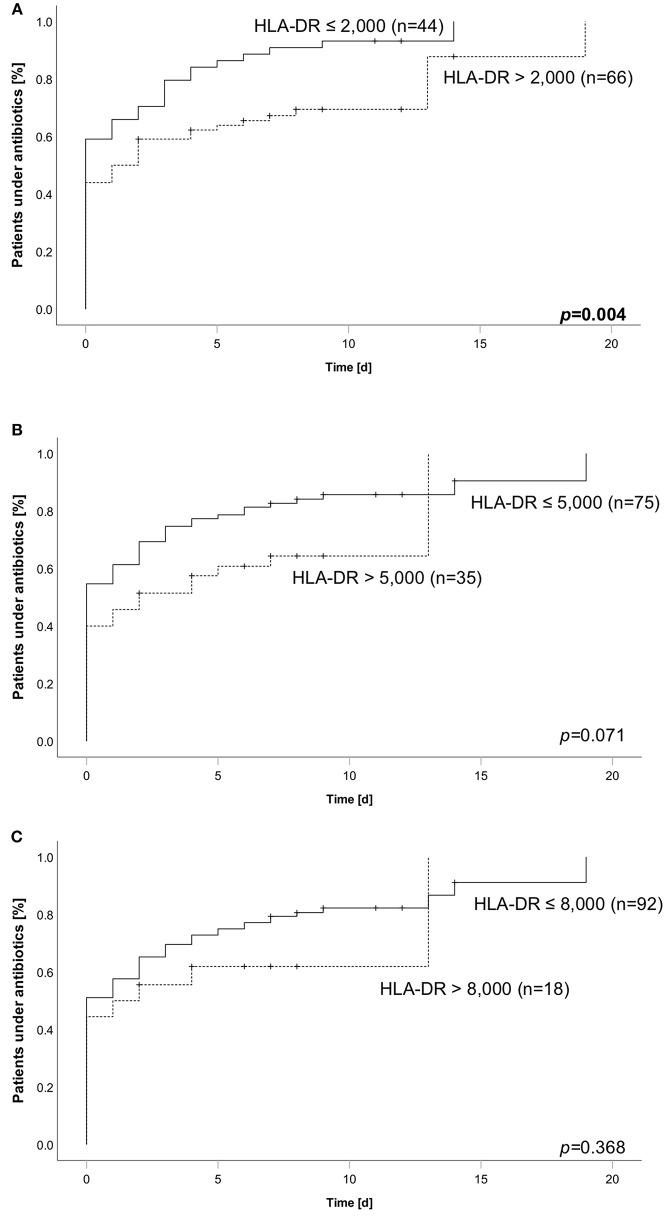
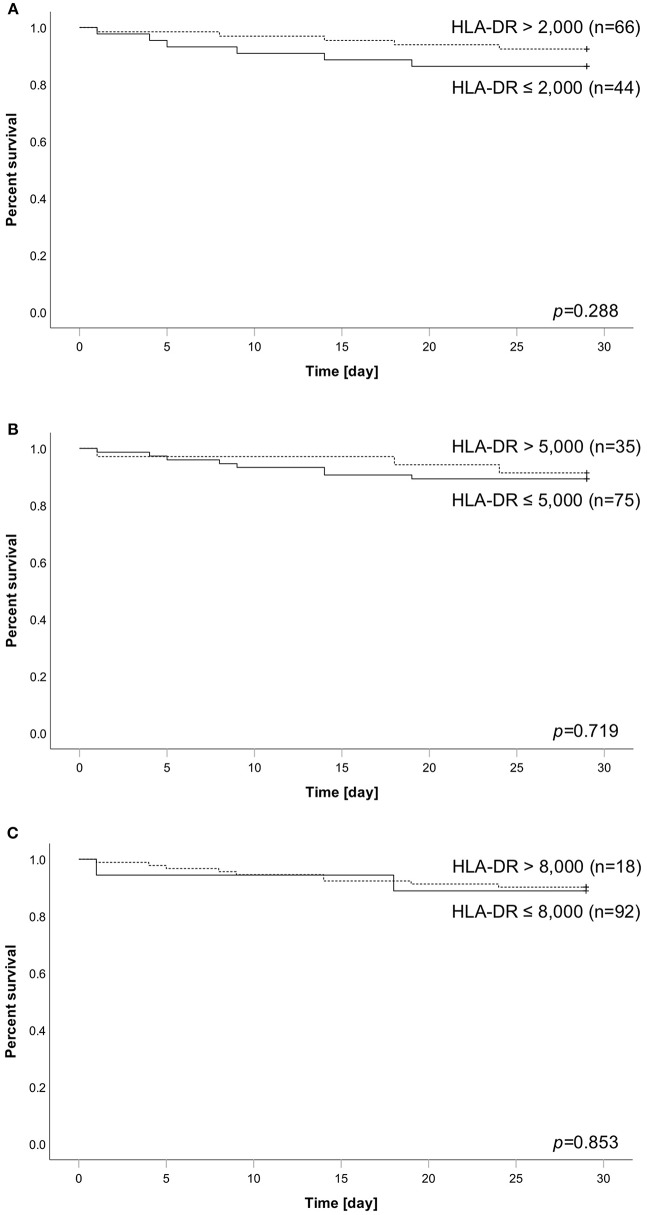
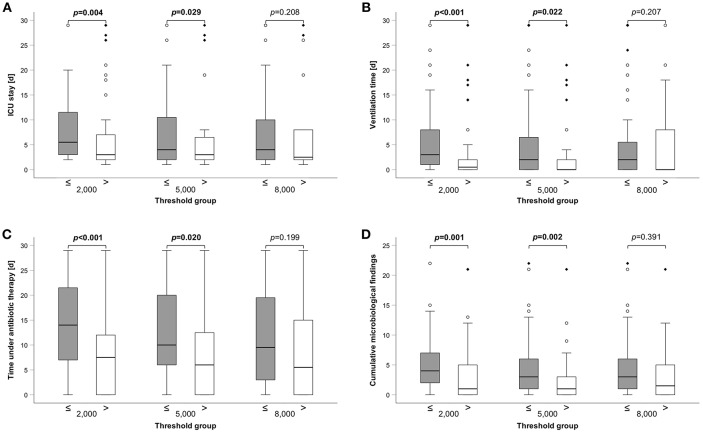
Critically ill patients, especially following trauma or extensive surgery, experience a systemic immune response, consisting of a pro-inflammatory as well as a counterbalancing anti-inflammatory response. Pro-inflammation is necessary for the initiation of homeostatic control and wound healing of the organism. However, when the counterbalancing mechanisms dominate, a condition of secondary immunodeficiency occurs, which renders the patient susceptible for opportunistic or secondary infections. However, the incidence of this condition is yet illusive. For a period of 3 months (May to July 2017), 110 consecutive patients admitted to the surgical ICU of the Heidelberg University Hospital, a tertiary university hospital, were enrolled in the study. Monocyte HLA-DR (mHLA-DR), a long-known surrogate of monocyte function, was assessed quantitatively once on admission utilizing a novel point-of-care flow cytometer with single-use cartridges (Accelix system). Patients were followed up for further 28 days and data on ICU stay, antibiotic therapy, microbiological findings, and mechanical ventilation were recorded. Statistical analysis was performed to evaluate the incidence of immunosuppression-defined by different thresholds-as well as its consequence in terms of outcome and clinical course. Depending on the HLA-DR threshold applied for stratification (≤8,000/≤5,000/≤2,000 molecules/cell), a large group of patients (85.5/68.2/40.0%) already presented with a robust decrease of HLA-DR on admission, independent of the cause for critical illness. Analyzed for survival, neither threshold was able to stratify patients with a higher mortality. However, both thresholds of 2,000 and 5,000 were able to discriminate patients with longer ICU stay, ventilation time and duration of antibiotic therapy, as well as higher count of microbiological findings. Moreover, a mHLA-DR value ≤2,000 molecules/cell was associated with higher incidence of overall antibiotic therapy. Single assessment of mHLA-DR using a novel point-of-care flow cytometer is able to stratify patients according to their risk of a complicated course. Therefore, this device overcomes the technical boundaries for measuring cellular biomarkers and paves the way for future studies involving personalized immunotherapy to patients with a high immunological risk profile independent of their background. German Clinical Trials Register; ID: DRKS00012348.
危重病患者,特别是在创伤或广泛手术后,会经历全身性免疫反应,包括促炎反应和抗炎反应的平衡。促炎反应对于启动机体的内稳态控制和伤口愈合是必要的。然而,当平衡机制占主导地位时,就会出现继发性免疫缺陷的情况,使患者容易发生机会性或继发性感染。然而,这种情况的发生率仍不清楚。在 2017 年 5 月至 7 月的 3 个月期间,共纳入了 110 例连续入住海德堡大学医院外科重症监护病房(三级大学医院)的患者。单核细胞 HLA-DR(mHLA-DR),单核细胞功能的长期已知替代物,在入院时利用带有一次性试剂盒的新型即时检测流式细胞仪进行定量评估(Accelix 系统)。对患者进行了 28 天的随访,并记录了 ICU 住院时间、抗生素治疗、微生物学发现和机械通气的数据。进行了统计学分析,以评估不同阈值定义的免疫抑制发生率,以及其在预后和临床过程方面的后果。根据 HLA-DR 分层应用的阈值(≤8000/≤5000/≤2000 分子/细胞),很大一部分患者(85.5%/68.2%/40.0%)在入院时已经出现 HLA-DR 的明显下降,与危重病的病因无关。对生存进行分析,没有一个阈值能够对死亡率较高的患者进行分层。然而,2000 和 5000 的两个阈值都能够区分 ICU 住院时间、通气时间和抗生素治疗时间较长的患者,以及微生物学发现计数较高的患者。此外,mHLA-DR 值≤2000 分子/细胞与更频繁使用总抗生素治疗相关。使用新型即时检测流式细胞仪对 mHLA-DR 进行单次评估,能够根据患者复杂病程的风险对患者进行分层。因此,该设备克服了测量细胞生物标志物的技术限制,为未来的研究铺平了道路,这些研究涉及对具有高免疫风险特征的患者进行个性化免疫治疗,而不受其背景的影响。德国临床试验注册处;注册号:DRKS00012348。