Department of Social Security, School of Labor and Human Resources, Renmin University of China, Beijing, China.
Department of Social and Behavioral Sciences, Harvard T.H. Chan School of Public Health, Boston, MA, USA.
Int J Equity Health. 2019 Mar 27;18(1):51. doi: 10.1186/s12939-019-0953-y.
Ensuring equitable access to medical care with financial risk protection has been at the center of achieving universal health coverage. In this paper, we assess the levels and trends of inequalities in medical care utilization and household catastrophic health spending (HCHS) at the national and sub-national levels in Rwanda.
Using the Rwanda Integrated Living Conditions Surveys of 2005, 2010, 2014, and 2016, we applied multivariable logit models to generate the levels and trends of adjusted inequalities in medical care utilization and HCHS across the four survey years by four socio-demographic dimensions: poverty, gender, education, and residence. We measured the national- and district-level inequalities in both absolute and relative terms.
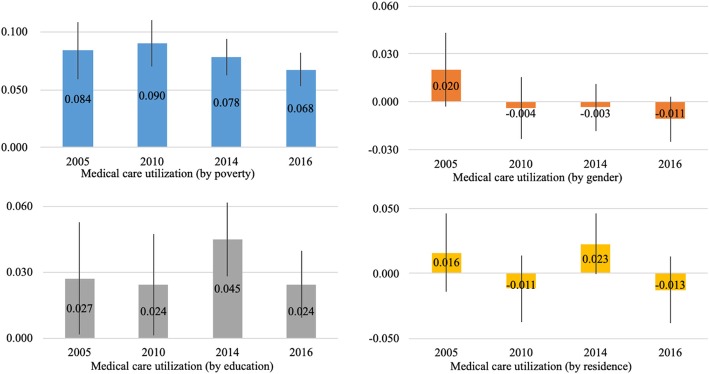
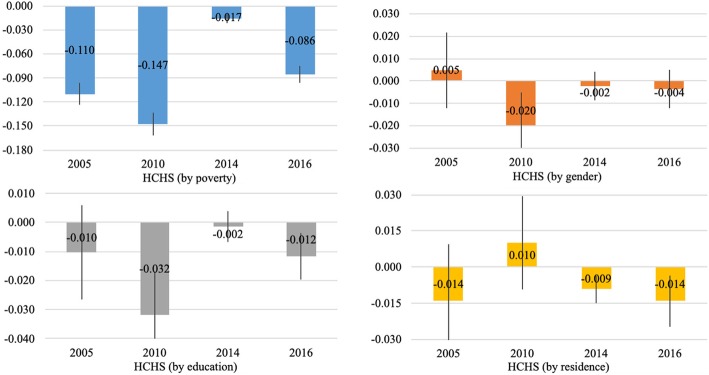
At the national level, after controlling for other factors, we found significant inequalities in medical care utilization by poverty and education and -in HCHS by poverty in all four years. From 2005 to 2016, inequalities in medical care utilization by the four dimensions did not change significantly, while the inequality in HCHS by poverty was reduced significantly. At the district level, inequalities in both medical care utilization and HCHS were larger than zero in all four years and decreased over time.
Poverty and poor education were significant contributors to inequalities in medical care utilization and HCHS in Rwanda. Policies or interventions targeting poor households or households headed by persons receiving no education are needed in order to effectively reduce inequalities in medical care utilization and HCHS.
确保在医疗保健方面享有公平的机会并提供财务风险保护,一直是实现全民健康覆盖的核心。本文旨在评估卢旺达在国家和次国家层面上医疗服务利用和家庭灾难性卫生支出(HCHS)不平等的程度和趋势。
利用 2005、2010、2014 和 2016 年的卢旺达综合生活状况调查数据,我们采用多变量逻辑回归模型,通过四个社会人口学维度(贫困、性别、教育和居住地),分析了四个调查年份医疗服务利用和 HCHS 调整后不平等的程度和趋势。我们从绝对值和相对值两个方面衡量了国家和地区层面的不平等。
在国家层面,在控制了其他因素后,我们发现医疗服务利用在贫困和教育方面存在显著的不平等,而 HCHS 在所有四年中都与贫困有关。2005 年至 2016 年期间,四个维度的医疗服务利用不平等没有显著变化,而贫困导致的 HCHS 不平等显著减少。在地区层面,所有四年的医疗服务利用和 HCHS 不平等均大于零,且随时间呈下降趋势。
贫困和教育程度低是卢旺达医疗服务利用和 HCHS 不平等的重要原因。需要针对贫困家庭或没有接受教育的家庭户主采取政策或干预措施,以有效减少医疗服务利用和 HCHS 的不平等。