Satyanarayana Srinath, Kwan Ada, Daniels Benjamin, Subbaraman Ramnath, McDowell Andrew, Bergkvist Sofi, Das Ranendra K, Das Veena, Das Jishnu, Pai Madhukar
McGill International Tuberculosis Centre & Department of Epidemiology, Biostatistics and Occupational Health, McGill University, Montreal, QC, Canada.
Development Research Group, The World Bank, Washington, DC, USA.
Lancet Infect Dis. 2016 Nov;16(11):1261-1268. doi: 10.1016/S1473-3099(16)30215-8. Epub 2016 Aug 25.
India's total antibiotic use is the highest of any country. Patients often receive prescription-only drugs directly from pharmacies. Here we aimed to assess the medical advice and drug dispensing practices of pharmacies for standardised patients with presumed and confirmed tuberculosis in India.
In this cross-sectional study in the three Indian cities Delhi, Mumbai, and Patna, we developed two standardised patient cases: first, a patient presenting with 2-3 weeks of pulmonary tuberculosis symptoms (Case 1); and second, a patient with microbiologically confirmed pulmonary tuberculosis (Case 2). Standardised patients were scheduled to present each case once to sampled pharmacies. We defined ideal management for both cases a priori as referral to a health-care provider without dispensing antibiotics or steroids or both.
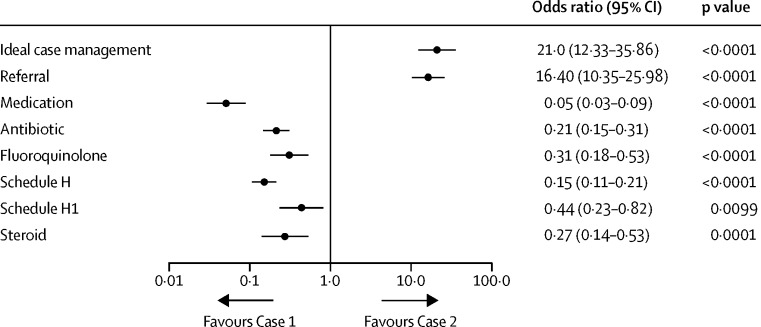
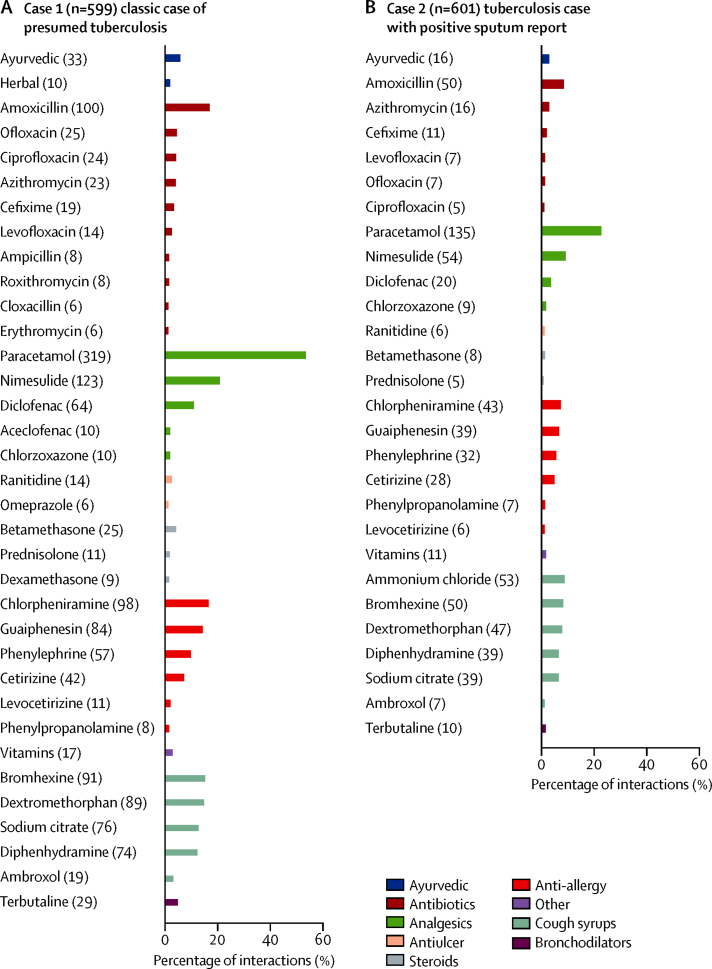
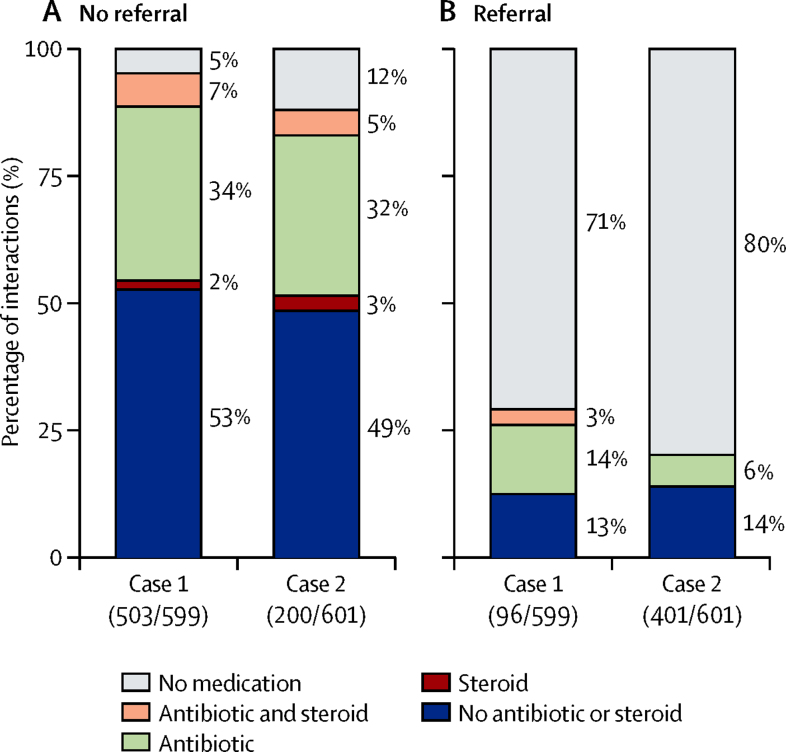
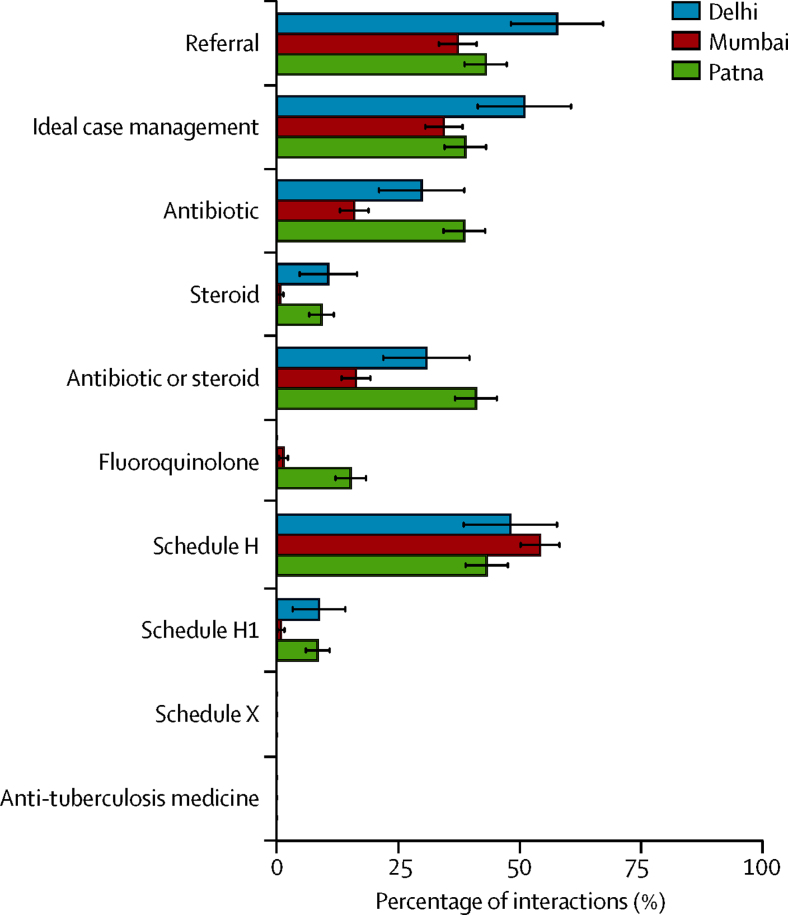
Between April 1, 2014, and Nov 29, 2015, we sampled 622 pharmacies in Delhi, Mumbai, and Patna. Standardised patients completed 1200 (96%) of 1244 interactions. We recorded ideal management (defined as referrals without the use of antibiotics or steroids) in 80 (13%) of 599 Case 1 interactions (95% CI 11-16) and 372 (62%) of 601 Case 2 interactions (95% CI 58-66). Antibiotic use was significantly lower in Case 2 interactions (98 [16%] of 601, 95% CI 13-19) than in Case 1 (221 [37%] of 599, 95% CI 33-41). First-line anti-tuberculosis drugs were not dispensed in any city. The differences in antibiotic or steroid use and number of medicines dispensed between Case 1 and Case 2 were almost entirely attributable to the difference in referral behaviour.
Only some urban Indian pharmacies correctly managed patients with presumed tuberculosis, but most correctly managed a case of confirmed tuberculosis. No pharmacy dispensed anti-tuberculosis drugs for either case. Absence of a confirmed diagnosis is a key driver of antibiotic misuse and could inform antimicrobial stewardship interventions.
Grand Challenges Canada, Bill & Melinda Gates Foundation, Knowledge for Change Program, and World Bank Development Research Group.
印度的抗生素总使用量在所有国家中是最高的。患者经常直接从药店获取仅凭处方才能购买的药品。在此,我们旨在评估印度药店针对疑似和确诊肺结核的标准化患者的医疗建议及药品配给做法。
在印度德里、孟买和巴特那这三个城市开展的这项横断面研究中,我们设计了两个标准化患者病例:其一,一名出现2至3周肺结核症状的患者(病例1);其二,一名经微生物学确诊的肺结核患者(病例2)。标准化患者按计划向抽样的药店各呈现一次每个病例。我们事先将两个病例的理想管理定义为转诊至医疗保健提供者,且不配发抗生素或类固醇或两者皆不配发。
在2014年4月1日至2015年11月29日期间,我们在德里、孟买和巴特那抽取了622家药店。标准化患者完成了1244次互动中的1200次(96%)。我们在599次病例1互动中的80次(13%)(95%置信区间11 - 16)以及601次病例2互动中的372次(62%)(95%置信区间58 - 66)记录到了理想管理(定义为不使用抗生素或类固醇的转诊)。病例2互动中的抗生素使用(601次中的98次[16%],95%置信区间13 - 19)显著低于病例1(599次中的221次[37%],95%置信区间33 - 41)。在任何一个城市都未配发出一线抗结核药物。病例1和病例2在抗生素或类固醇使用以及配给药品数量上的差异几乎完全归因于转诊行为的差异。
印度只有部分城市药店正确管理了疑似肺结核患者,但大多数正确管理了确诊肺结核病例。没有一家药店为任何一个病例配发出抗结核药物。缺乏确诊诊断是抗生素滥用的关键驱动因素,可为抗菌药物管理干预提供依据。
加拿大重大挑战项目、比尔及梅琳达·盖茨基金会、知识促进变革项目以及世界银行发展研究小组。