Szummer Karolina, Gasparini Alessandro, Eliasson Staffan, Ärnlöv Johan, Qureshi Abdul Rashid, Bárány Peter, Evans Marie, Friberg Leif, Carrero Juan Jesus
Department of Medicine, Karolinska Institutet, Stockholm, Sweden
Department of Cardiology, Karolinska University Hospital, Stockholm, Sweden.
J Am Heart Assoc. 2017 Mar 1;6(3):e004925. doi: 10.1161/JAHA.116.004925.
It is unknown whether renal dysfunction conveys poor anticoagulation control in warfarin-treated patients with atrial fibrillation and whether poor anticoagulation control associates with the risk of adverse outcomes in these patients.
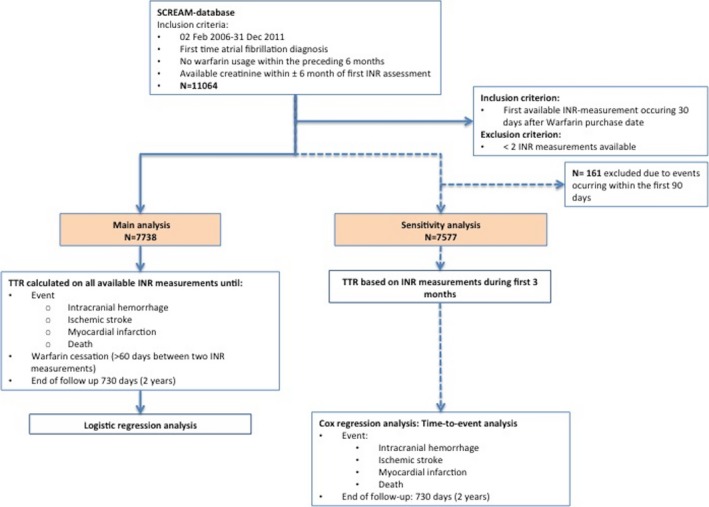
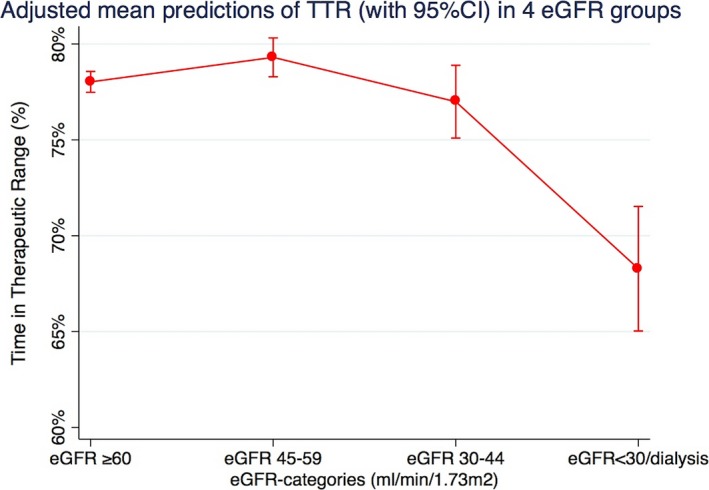
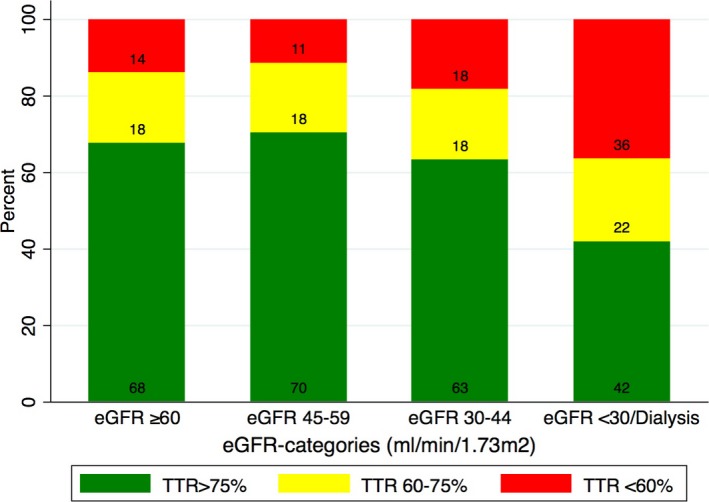
This was an observational study from the Stockholm CREatinine Measurements (SCREAM) cohort including all newly diagnosed atrial fibrillation patients initiating treatment with warfarin (n=7738) in Stockholm, Sweden, between 2006 and 2011. Estimated glomerular filtration rate (eGFR; mL/min per 1.73 m) was calculated from serum creatinine. Time-in-therapeutic range (TTR) was assessed from international normalized ratio (INR) measurements up to warfarin cessation, adverse event, or end of follow-up (2 years). Adverse events considered a composite of intracranial hemorrhage, ischemic stroke, myocardial infarction, or death. During median 254 days, TTR was 83%, based on median 21 INR measurements per patient. TTR was 70% among patients with eGFR <30, around 10% lower than in those with normal renal function. During observation, adverse events occurred in 4.0% of patients, and those with TTR ≤75% were at higher adverse event risk. This was independent of patient characteristics, comorbidities, number of INR tests, days exposed to warfarin, and, notably, independent of eGFR: adjusted odds ratio (OR) 1.84 (95% CI, 1.41-2.40) for TTR 75% to 60% and adjusted OR 2.09 (1.59-2.74) for TTR <60%. No interaction was observed between eGFR and TTR in association to adverse events (=0.2).
Severe chronic kidney disease (eGFR <30) patients with atrial fibrillation have worse INR control while on warfarin. An optimal TTR (>75%) is associated with lower risk of adverse events, independently of underlying renal function.
在接受华法林治疗的房颤患者中,肾功能不全是否会导致抗凝控制不佳,以及抗凝控制不佳是否与这些患者的不良结局风险相关尚不清楚。
这是一项来自斯德哥尔摩肌酐测量(SCREAM)队列的观察性研究,纳入了2006年至2011年期间在瑞典斯德哥尔摩所有新诊断的开始接受华法林治疗的房颤患者(n = 7738)。根据血清肌酐计算估算肾小球滤过率(eGFR;每1.73平方米的毫升/分钟)。从国际标准化比值(INR)测量值评估至华法林停药、不良事件或随访结束(2年)的治疗范围内时间(TTR)。不良事件被视为颅内出血、缺血性中风、心肌梗死或死亡的综合事件。在中位254天期间,基于每位患者中位21次INR测量,TTR为83%。eGFR<30的患者中TTR为70%,比肾功能正常的患者低约10%。在观察期间,4.0%的患者发生了不良事件,TTR≤75%的患者不良事件风险更高。这与患者特征、合并症、INR检测次数、暴露于华法林的天数无关,尤其与eGFR无关:TTR为75%至60%时调整后的比值比(OR)为1.84(95%CI,1.41 - 2.40),TTR<60%时调整后的OR为2.09(1.59 - 2.74)。在与不良事件的关联中,未观察到eGFR与TTR之间的相互作用(P = 0.2)。
房颤合并严重慢性肾病(eGFR<30)的患者在服用华法林时INR控制较差。最佳TTR(>75%)与较低的不良事件风险相关,与潜在肾功能无关。