Mohd Hanafiah Khayriyyah, Garcia Mary Louise, Anderson David Andrew
Life Sciences, Macfarlane Burnet Institute, Melbourne 3004, Victoria, Australia.
School of Biological Sciences, Universiti Sains Malaysia, Pulau Pinang 11600, Malaysia.
Trop Med Infect Dis. 2019 Mar 31;4(2):57. doi: 10.3390/tropicalmed4020057.
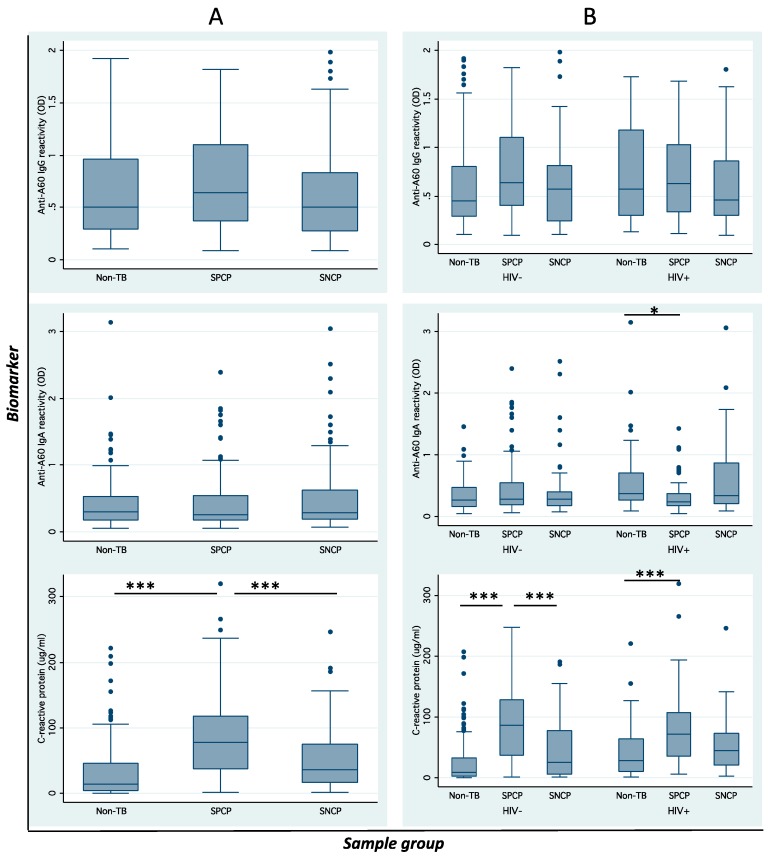
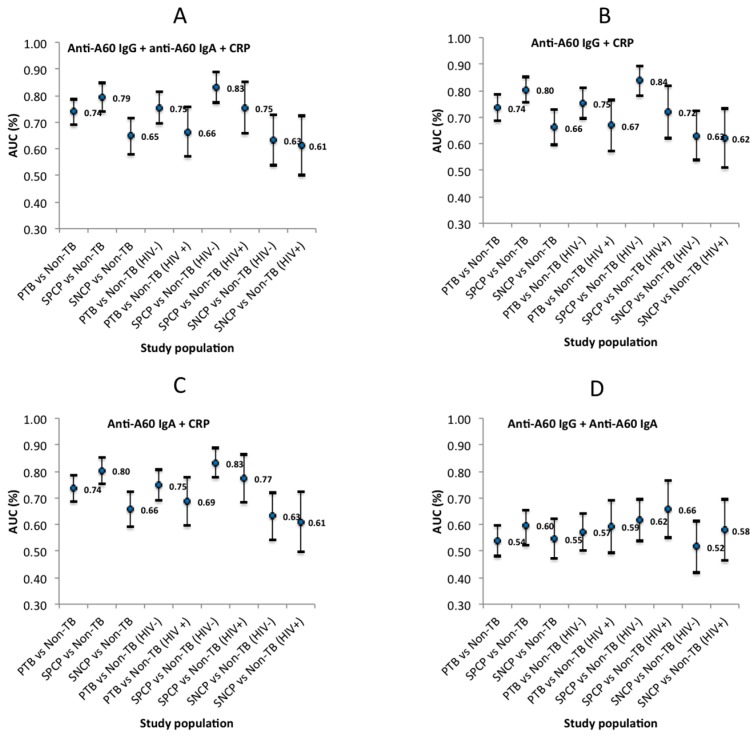
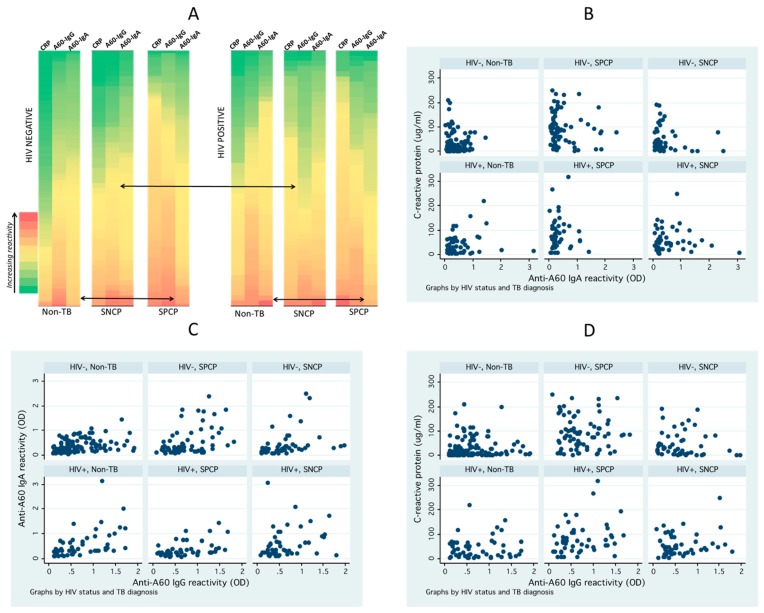
Influence of host factors, including human immunodeficiency virus (HIV) co-infection, on the distribution and diagnostic potential of previously evaluated biomarkers of pulmonary tuberculosis (PTB), such as anti-antigen 60 (A60) immunoglobulin (Ig) G, anti-A60 IgA, and C-reactive protein (CRP), remain unclear. Anti-A60 IgG, anti-A60 IgA, and CRP in PTB and non-PTB patient sera ( = 404, including smear-positive/negative, culture-positive (SPCP/SNCP) and HIV+ve/-ve) were measured by enzyme-linked immunoassay and statistically analysed. In multinomial logistic regression, expectoration, chest pain, wasting, and culture count positively associated with CRP ( < 0.001), while smear count positively associated with anti-A60 IgG ( = 0.090). Expectoration and enlarged lymph nodes negatively associated with anti-A60 IgA ( = 0.018). Biomarker distribution and diagnostic potential varied significantly by symptoms and bacilli burden, and across different PTB subpopulations. CRP was correlated poorly with anti-A60 antibodies, while anti-A60 IgA and IgG were correlated in non-tuberculosis (TB) and SPCP patients ( < 0.001). When combined, anti-A60 IgG and CRP best discriminated SPCP/HIV-ve from non-TB (AUC: 0.838, 95% CI: 0.783⁻0.894), while anti-A60 IgA and CRP performed best in discriminating HIV+ve PTB from non-TB (AUC: 0.687, 95% CI: 0.598⁻0.777). Combined CRP and anti-A60 antibodies had significantly reduced accuracy in SNCP and SNCP/HIV+ve compared to SPCP/HIV-ve subpopulations. The complex relationships between host factors and biomarkers suggest their limited utility, especially in SNCP/HIV+ve subpopulations, highlighting the importance of examining host response and immune biomarkers across relevant patient subpopulations.
包括人类免疫缺陷病毒(HIV)合并感染在内的宿主因素对先前评估的肺结核(PTB)生物标志物(如抗抗原60(A60)免疫球蛋白(Ig)G、抗A60 IgA和C反应蛋白(CRP))的分布及诊断潜力的影响仍不明确。通过酶联免疫吸附测定法检测并统计分析了PTB和非PTB患者血清(n = 404,包括涂片阳性/阴性、培养阳性(SPCP/SNCP)以及HIV阳性/阴性)中的抗A60 IgG、抗A60 IgA和CRP。在多项逻辑回归分析中,咳痰、胸痛、消瘦和培养菌数与CRP呈正相关(P < 0.001),而涂片菌数与抗A60 IgG呈正相关(P = 0.090)。咳痰和淋巴结肿大与抗A60 IgA呈负相关(P = 0.018)。生物标志物的分布和诊断潜力因症状和杆菌负荷不同,以及在不同的PTB亚组中存在显著差异。CRP与抗A60抗体的相关性较差,而抗A60 IgA和IgG在非结核(TB)和SPCP患者中存在相关性(P < 0.001)。联合使用时,抗A60 IgG和CRP在区分SPCP/HIV阴性与非结核方面表现最佳(曲线下面积(AUC):0.838,95%置信区间(CI):0.783⁻0.894),而抗A60 IgA和CRP在区分HIV阳性PTB与非结核方面表现最佳(AUC:0.687,95% CI:0.598⁻0.777)。与SPCP/HIV阴性亚组相比,联合CRP和抗A60抗体在SNCP和SNCP/HIV阳性亚组中的准确性显著降低。宿主因素与生物标志物之间的复杂关系表明它们的效用有限,尤其是在SNCP/HIV阳性亚组中,这凸显了在相关患者亚组中研究宿主反应和免疫生物标志物的重要性。