Hummel James P, Leipold Robert J, Amorosi Stacey L, Bao Haikun, Deger Kristen A, Jones Paul W, Kansal Anuraag R, Ott Lesli S, Stern Sean, Stein Kenneth, Curtis Jeptha P, Akar Joseph G
Division of Cardiology, University of Wisconsin School of Medicine and Public Health, Madison, Wisconsin.
Evidera, Bethesda, Maryland.
J Cardiovasc Electrophysiol. 2019 Jul;30(7):1066-1077. doi: 10.1111/jce.13934. Epub 2019 Apr 29.
Remote monitoring of implantable cardioverter-defibrillators has been associated with reduced rates of all-cause rehospitalizations and mortality among device recipients, but long-term economic benefits have not been studied.
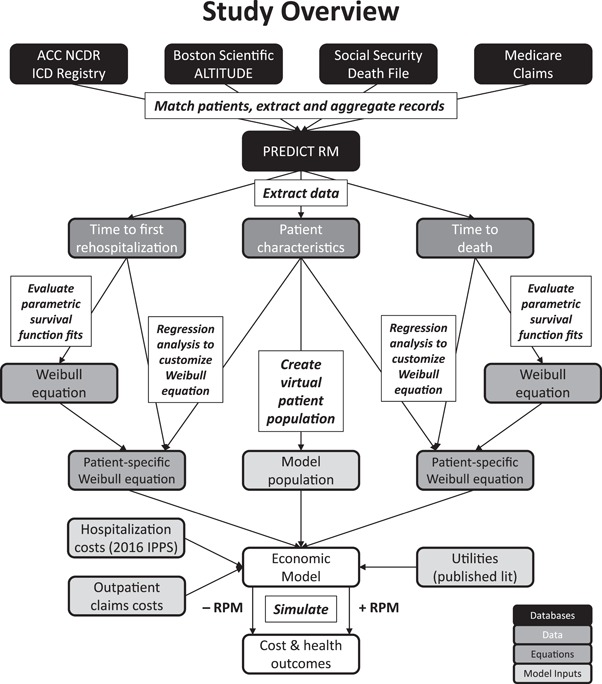
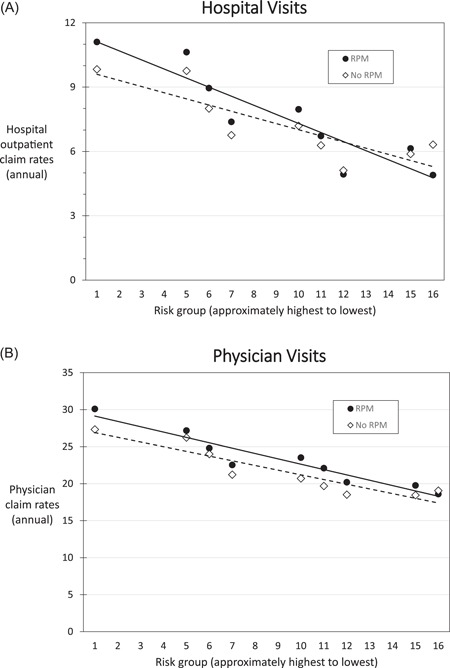
An economic model was developed using the PREDICT RM database comparing outcomes with and without remote monitoring. The database included patients ages 65 to 89 who received a Boston Scientific device from 2006 to 2010. Parametric survival equations were derived for rehospitalization and mortality to predict outcomes over a maximum time horizon of 25 years. The analysis assessed rehospitalization, mortality, and the cost-effectiveness (expressed as the incremental cost per quality-adjusted life year) of remote monitoring versus no remote monitoring. Remote monitoring was associated with reduced mortality; average life expectancy and average quality-adjusted life years increased by 0.77 years and 0.64, respectively (6.85 life years and 5.65 quality-adjusted life years). When expressed per patient-year, remote monitoring patients had fewer subsequent rehospitalizations (by 0.08 per patient-year) and lower hospitalization costs (by $554 per patient year). With longer life expectancies, remote monitoring patients experienced an average of 0.64 additional subsequent rehospitalizations with increased average lifetime hospitalization costs of $2784. Total costs of outpatient and physician claims were higher with remote monitoring ($47 515 vs $42 792), but average per patient-year costs were lower ($6232 vs $6244). The base-case incremental cost-effectiveness ratio was $10 752 per quality-adjusted life year, making remote monitoring high-value care.
Remote monitoring is a cost-effective approach for the lifetime management of patients with implantable cardioverter-defibrillators.
植入式心脏复律除颤器的远程监测与降低器械植入者的全因再住院率和死亡率相关,但长期经济效益尚未得到研究。
使用PREDICT RM数据库建立了一个经济模型,比较有远程监测和无远程监测的结果。该数据库包括2006年至2010年期间接受波士顿科学公司器械的65至89岁患者。推导了再住院和死亡率的参数生存方程,以预测最长25年时间范围内的结果。该分析评估了远程监测与无远程监测相比的再住院率、死亡率和成本效益(以每质量调整生命年的增量成本表示)。远程监测与死亡率降低相关;平均预期寿命和平均质量调整生命年分别增加了0.77年和0.64年(6.85个生命年和5.65个质量调整生命年)。按患者年计算,接受远程监测的患者后续再住院次数较少(每位患者每年少0.08次),住院费用较低(每位患者每年少554美元)。随着预期寿命延长,接受远程监测的患者平均额外有0.64次后续再住院,平均终身住院费用增加2784美元。远程监测的门诊和医生索赔总费用较高(47515美元对42792美元),但每位患者每年的平均费用较低(6232美元对6244美元)。基础病例增量成本效益比为每质量调整生命年10752美元,这使得远程监测成为高价值医疗。
远程监测是植入式心脏复律除颤器患者终身管理的一种具有成本效益的方法。