Division of Cardiology, Johns Hopkins School of Medicine, Baltimore, Maryland, United States of America.
Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, United States of America.
PLoS One. 2019 Apr 4;14(4):e0214735. doi: 10.1371/journal.pone.0214735. eCollection 2019.
HIV-infected persons have an increased risk of atherosclerosis relative to uninfected individuals. Inflammatory processes may contribute to this risk. We evaluated the associations of 10 biomarkers of systemic inflammation (CRP, IL-6, sTNF-αR1 and 2), monocyte activation (CCL2, sCD163, sCD14), coagulation (fibrinogen, D-dimer), and endothelial dysfunction (ICAM-1) with subclinical carotid atherosclerosis among participants in the Multicenter AIDS Cohort Study (MACS).
Carotid plaque and intima media thickness (IMT) in the common carotid (CCA-IMT) and bifurcation region were assessed by B mode ultrasound among 452 HIV-infected and 276 HIV-uninfected men from 2010-2013. Associations between levels of each biomarker and presence of focal plaque and IMT were assessed by logistic and linear regression models, adjusting for demographics, risk behaviors, traditional cardiovascular disease (CVD) risk factors, and HIV disease characteristics.
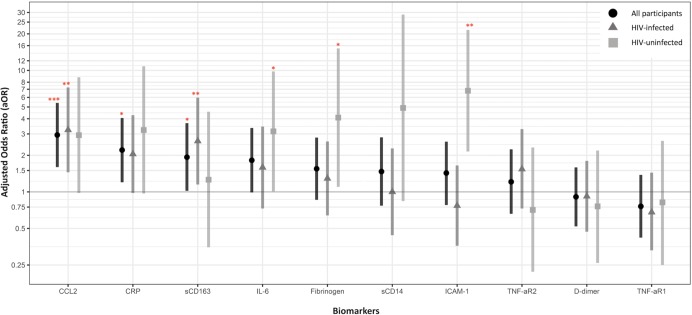
Compared to HIV-uninfected men, HIV-infected men had significantly higher levels of 8 of the 10 biomarkers. Overall, men with sCD163, CCL2, IL-6, and CRP levels in the highest quintile had approximately 2 times the odds of carotid plaque relative to those with levels in the lowest quintile, independent of demographic and CVD risk factors. Fibrinogen levels were positively associated with CCA-IMT while ICAM-1, CCL2, and sTNF-αR1 levels were positively associated with bifurcation-IMT. Among HIV-uninfected men, higher levels of sTNF-αR2 were positively associated with CCA-IMT, fibrinogen with bifurcation-IMT and carotid plaque, and ICAM-1 with carotid plaque.
In addition to greater levels of systemic inflammation, heightened monocyte activation (sCD163, CCL2) may contribute to the burden of atherosclerosis among HIV-infected persons.
与未感染个体相比,HIV 感染者发生动脉粥样硬化的风险增加。炎症过程可能导致这种风险。我们评估了 10 种全身炎症生物标志物(CRP、IL-6、sTNF-αR1 和 2)、单核细胞活化(CCL2、sCD163、sCD14)、凝血(纤维蛋白原、D-二聚体)和内皮功能障碍(ICAM-1)与多中心 AIDS 队列研究(MACS)参与者亚临床颈动脉粥样硬化的相关性。
2010-2013 年间,通过 B 型超声评估了 452 名 HIV 感染者和 276 名 HIV 未感染者的颈总动脉(CCA-IMT)和分叉区的颈动脉斑块和内膜中层厚度(IMT)。使用逻辑回归和线性回归模型评估了每种生物标志物水平与局灶性斑块和 IMT 存在之间的关系,调整了人口统计学、风险行为、传统心血管疾病(CVD)危险因素和 HIV 疾病特征。
与 HIV 未感染者相比,HIV 感染者的 10 种生物标志物中有 8 种的水平显著升高。总体而言,sCD163、CCL2、IL-6 和 CRP 水平处于最高五分位的男性发生颈动脉斑块的几率是最低五分位的男性的大约 2 倍,独立于人口统计学和 CVD 危险因素。纤维蛋白原水平与 CCA-IMT 呈正相关,而 ICAM-1、CCL2 和 sTNF-αR1 水平与分叉-IMT 呈正相关。在 HIV 未感染者中,sTNF-αR2 水平升高与 CCA-IMT 呈正相关,纤维蛋白原与分叉-IMT 和颈动脉斑块呈正相关,ICAM-1 与颈动脉斑块呈正相关。
除了全身炎症水平较高外,单核细胞活化(sCD163、CCL2)的增加可能导致 HIV 感染者的动脉粥样硬化负担增加。