National Heart Lung Institute, Imperial College London, Emmanuel Kaye Building, 1b Manresa Road, London, SW3 6LR, UK.
Department of Statistical Science, University College London, London, UK.
BMC Med. 2019 Apr 5;17(1):73. doi: 10.1186/s12916-019-1310-0.
Chronic obstructive pulmonary disease (COPD) is a major cause of mortality. Patients with advanced disease often have a poor quality of life, such that guidelines recommend providing palliative care in their last year of life. Uptake and use of palliative care in advanced COPD is low; difficulty in predicting 1-year mortality is thought to be a major contributing factor.
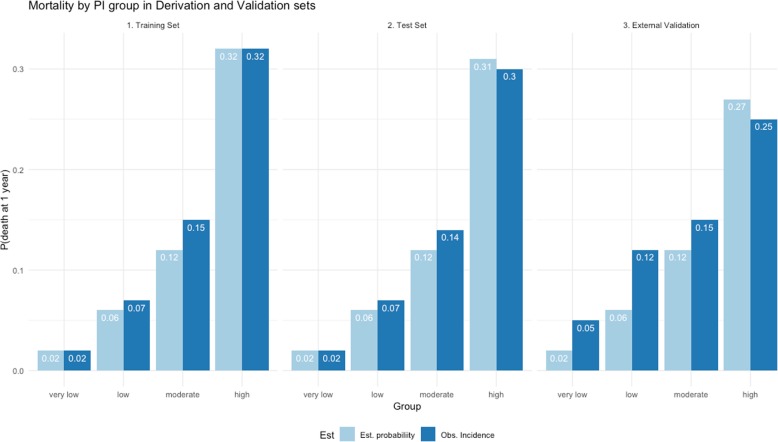
We identified two primary care COPD cohorts using UK electronic healthcare records (Clinical Practice Research Datalink). The first cohort was randomised equally into training and test sets. An external dataset was drawn from a second cohort. A risk model to predict mortality within 12 months was derived from the training set using backwards elimination Cox regression. The model was given the acronym BARC based on putative prognostic factors including body mass index and blood results (B), age (A), respiratory variables (airflow obstruction, exacerbations, smoking) (R) and comorbidities (C). The BARC index predictive performance was validated in the test set and external dataset by assessing calibration and discrimination. The observed and expected probabilities of death were assessed for increasing quartiles of mortality risk (very low risk, low risk, moderate risk, high risk). The BARC index was compared to the established index scores body mass index, obstructive, dyspnoea and exacerbations (BODEx), dyspnoea, obstruction, smoking and exacerbations (DOSE) and age, dyspnoea and obstruction (ADO).
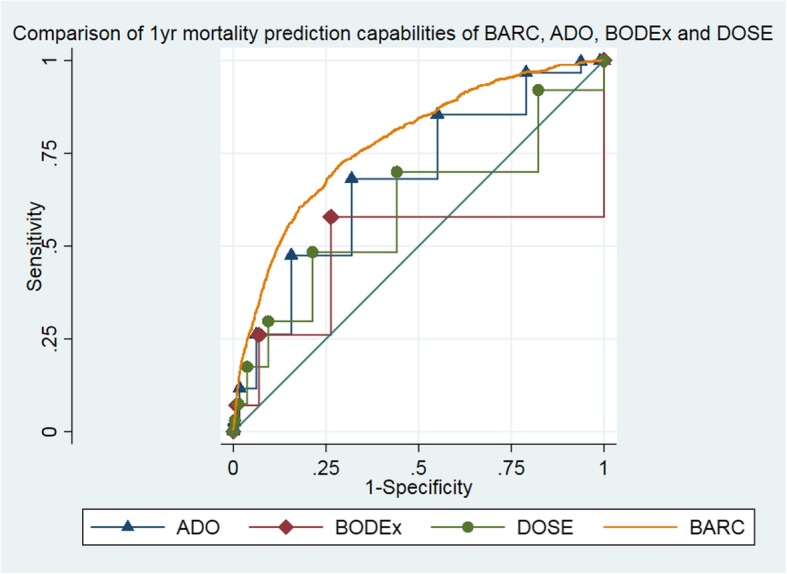
Fifty-four thousand nine hundred ninety patients were eligible from the first cohort and 4931 from the second cohort. Eighteen variables were included in the BARC, including age, airflow obstruction, body mass index, smoking, exacerbations and comorbidities. The risk model had acceptable predictive performance (test set: C-index = 0.79, 95% CI 0.78-0.81, D-statistic = 1.87, 95% CI 1.77-1.96, calibration slope = 0.95, 95% CI 0.9-0.99; external dataset: C-index = 0.67, 95% CI 0.65-0.7, D-statistic = 0.98, 95% CI 0.8-1.2, calibration slope = 0.54, 95% CI 0.45-0.64) and acceptable accuracy predicting the probability of death (probability of death in 1 year, n high-risk group, test set: expected = 0.31, observed = 0.30; external dataset: expected = 0.22, observed = 0.27). The BARC compared favourably to existing index scores that can also be applied without specialist respiratory variables (area under the curve: BARC = 0.78, 95% CI 0.76-0.79; BODEx = 0.48, 95% CI 0.45-0.51; DOSE = 0.60, 95% CI 0.57-0.61; ADO = 0.68, 95% CI 0.66-0.69, external dataset: BARC = 0.70, 95% CI 0.67-0.72; BODEx = 0.41, 95% CI 0.38-0.45; DOSE = 0.52, 95% CI 0.49-0.55; ADO = 0.57, 95% CI 0.54-0.60).
The BARC index performed better than existing tools in predicting 1-year mortality. Critically, the risk score only requires routinely collected non-specialist information which, therefore, could help identify patients seen in primary care that may benefit from palliative care.
慢性阻塞性肺疾病(COPD)是主要的死亡原因之一。晚期疾病患者的生活质量往往较差,因此指南建议在生命的最后一年提供姑息治疗。晚期 COPD 患者接受姑息治疗的比例和使用率均较低;难以预测 1 年死亡率被认为是主要的促成因素。
我们使用英国电子医疗记录(临床实践研究数据链接)识别了两个初级保健 COPD 队列。第一个队列被平均分为训练集和测试集。第二个队列的数据取自外部数据集。使用向后消除 Cox 回归从训练集中推导出预测 12 个月内死亡率的风险模型。该模型基于可能的预后因素(包括体重指数和血液结果(B)、年龄(A)、呼吸变量(气流阻塞、加重、吸烟)(R)和合并症(C))的缩写为 BARC。在测试集和外部数据集中验证了 BARC 指数的预测性能,通过评估校准和区分来评估。评估了死亡风险增加的四个四分位数(极低风险、低风险、中风险、高风险)的观察到的和预期的死亡概率。将 BARC 指数与已建立的指数评分(体重指数、阻塞、呼吸困难和加重(BODEx)、呼吸困难、阻塞、吸烟和加重(DOSE)和年龄、呼吸困难和阻塞(ADO))进行了比较。
从第一个队列中选出了 54990 名符合条件的患者,从第二个队列中选出了 4931 名患者。BARC 中包含了 18 个变量,包括年龄、气流阻塞、体重指数、吸烟、加重和合并症。风险模型具有可接受的预测性能(测试集:C 指数=0.79,95%CI 0.78-0.81,D 统计量=1.87,95%CI 1.77-1.96,校准斜率=0.95,95%CI 0.9-0.99;外部数据集:C 指数=0.67,95%CI 0.65-0.7,D 统计量=0.98,95%CI 0.8-1.2,校准斜率=0.54,95%CI 0.45-0.64)和可接受的预测死亡概率的准确性(1 年的死亡概率,高风险组的 n,测试集:预期=0.31,观察=0.30;外部数据集:预期=0.22,观察=0.27)。BARC 与其他现有的指数评分相比表现良好,这些评分也可以在没有专门的呼吸变量的情况下应用(曲线下面积:BARC=0.78,95%CI 0.76-0.79;BODEx=0.48,95%CI 0.45-0.51;DOSE=0.60,95%CI 0.57-0.61;ADO=0.68,95%CI 0.66-0.69,外部数据集:BARC=0.70,95%CI 0.67-0.72;BODEx=0.41,95%CI 0.38-0.45;DOSE=0.52,95%CI 0.49-0.55;ADO=0.57,95%CI 0.54-0.60)。
BARC 指数在预测 1 年死亡率方面优于现有的工具。至关重要的是,风险评分只需要常规收集非专业信息,因此,这可能有助于识别在初级保健中接受姑息治疗的患者。