Chen Peipei, Chen Xi, Zhang Shuyang
Department of Cardiology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China.
Front Physiol. 2019 Mar 20;10:280. doi: 10.3389/fphys.2019.00280. eCollection 2019.
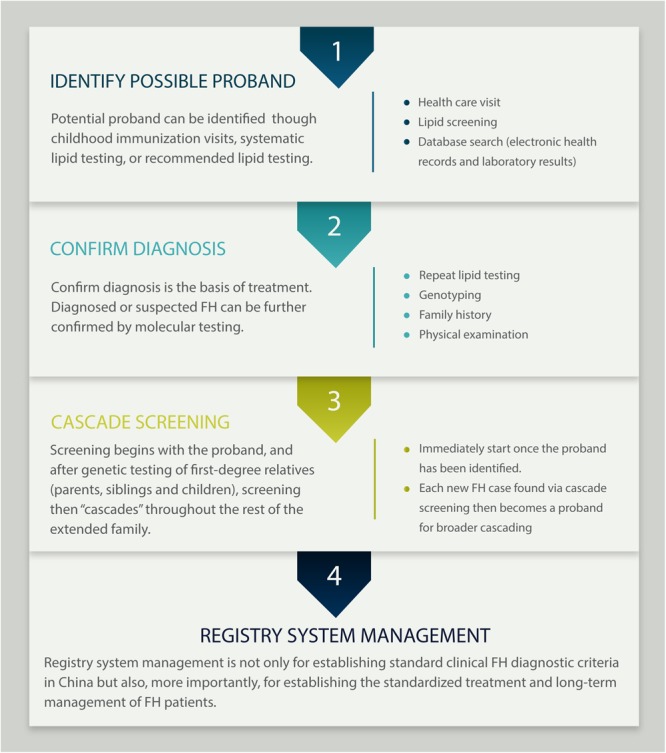
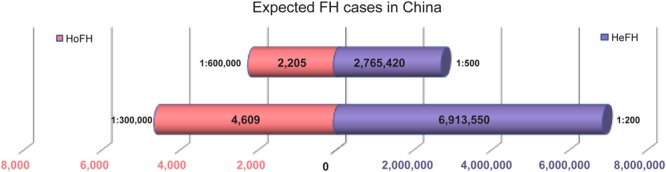
Familial hypercholesterolemia (FH) greatly facilitates the development of cardiovascular disease (CVD). Without timely treatment, the incidence of coronary heart disease (CHD) in patients with FH is 3 to 4 times that in non-FH patients, and the onset of CVD would be advanced by approximately 10 years. There is ample evidence that the diagnosis and adequate treatment of FH are not properly considered for all ethnicities. The monogenic cause of FH includes apolipoprotein B (APOB), low-density lipoprotein receptor (LDLR), and proprotein convertase subtilisin/kexin 9 (PCSK9). There are approximately 2,765,420 to 6,913,550 cases of potential heterozygous FH (HeFH) and 2,205 to 4,609 cases of potential homozygous FH (HoFH) in China. Nevertheless, China lacks clinical diagnostic criteria specific to Chinese patients, such that most FH patients cannot be diagnosed until middle age or after their first cardiovascular event, thus precluding early treatment. This article explores the gene mutations, diagnosis and treatment of FH patients in China. Following the implementation of the two-child policy, there is a need to establish Chinese FH registry systems and genetic databases and to address the challenges in conducting cascade screening and long-term management. Advocating the establishment of FH registry systems and databases is an important rate-limiting step in improving long-term prognosis in FH patients, so that joint efforts of clinical experts and public communities are required. We recommend a process flow from case identification to entry into the registry system, and the widespread use of the system in clinical applications can provide the best treatment guidance for medical practice.
家族性高胆固醇血症(FH)极大地促进了心血管疾病(CVD)的发展。若不及时治疗,FH患者冠心病(CHD)的发病率是非FH患者的3至4倍,且CVD的发病时间会提前约10年。有充分证据表明,并非所有种族都能充分考虑FH的诊断和适当治疗。FH的单基因病因包括载脂蛋白B(APOB)、低密度脂蛋白受体(LDLR)和前蛋白转化酶枯草溶菌素/kexin 9(PCSK9)。中国约有2,765,420至6,913,550例潜在杂合子FH(HeFH)病例以及2,205至4,609例潜在纯合子FH(HoFH)病例。然而,中国缺乏针对中国患者的临床诊断标准,以至于大多数FH患者直到中年或首次发生心血管事件后才能被诊断出来,从而无法进行早期治疗。本文探讨了中国FH患者的基因突变、诊断和治疗。随着二孩政策的实施,有必要建立中国FH登记系统和基因数据库,并应对开展级联筛查和长期管理方面的挑战。倡导建立FH登记系统和数据库是改善FH患者长期预后的重要限速步骤,因此需要临床专家和公众共同努力。我们推荐一个从病例识别到进入登记系统的流程,并且该系统在临床应用中的广泛使用可为医疗实践提供最佳治疗指导。