IRD UMI 233, INSERM U1175, Université de Montpellier, Unité TransVIHMI, 911 Avenue Agropolis, P.O. Box 64501, 34394, Montpellier, France.
Programme National de Lutte contre les Maladies Tropicales Négligées à Chimiothérapie Préventive, Ministère de la Santé Publique, 36, Avenue de la Justice, C/Gombe, Kinshasa, Democratic Republic of the Congo.
Parasit Vectors. 2019 Apr 11;12(1):162. doi: 10.1186/s13071-019-3428-5.
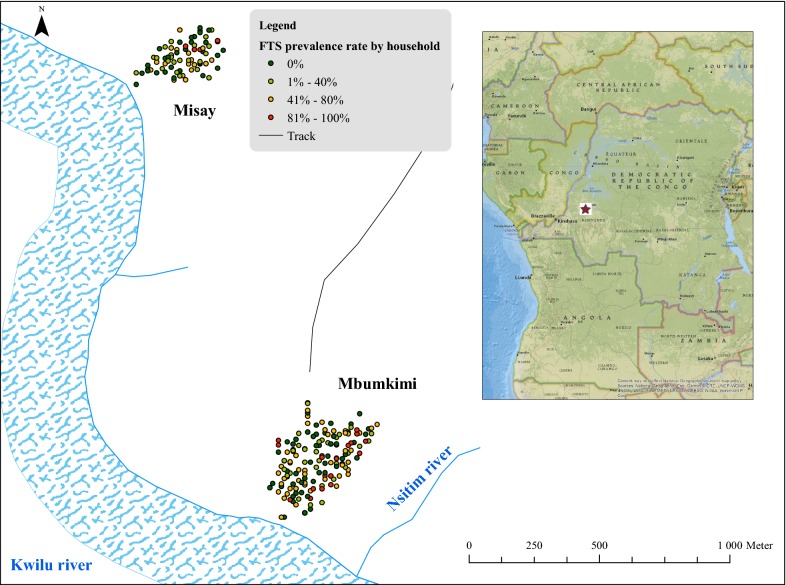
Little is known regarding risk factors for lymphatic filariasis (LF) in Central Africa. To expand on what is known, we studied the epidemiology of LF in two endemic villages in the Democratic Republic of the Congo.
Dependent variables were Wuchereria bancrofti antigenaemia detected with filarial test strips (FTS) and microfilaraemia detected by night blood smears. The following factors were investigated: sex, age, the use of bednets, the use of latrines, hunting, fishing and agricultural activities, history of treatment with anthelmintic drugs, overnight stays in the bush, population density, the number of household members, and distance to rivers. Mixed multivariate logistic regression models were used.
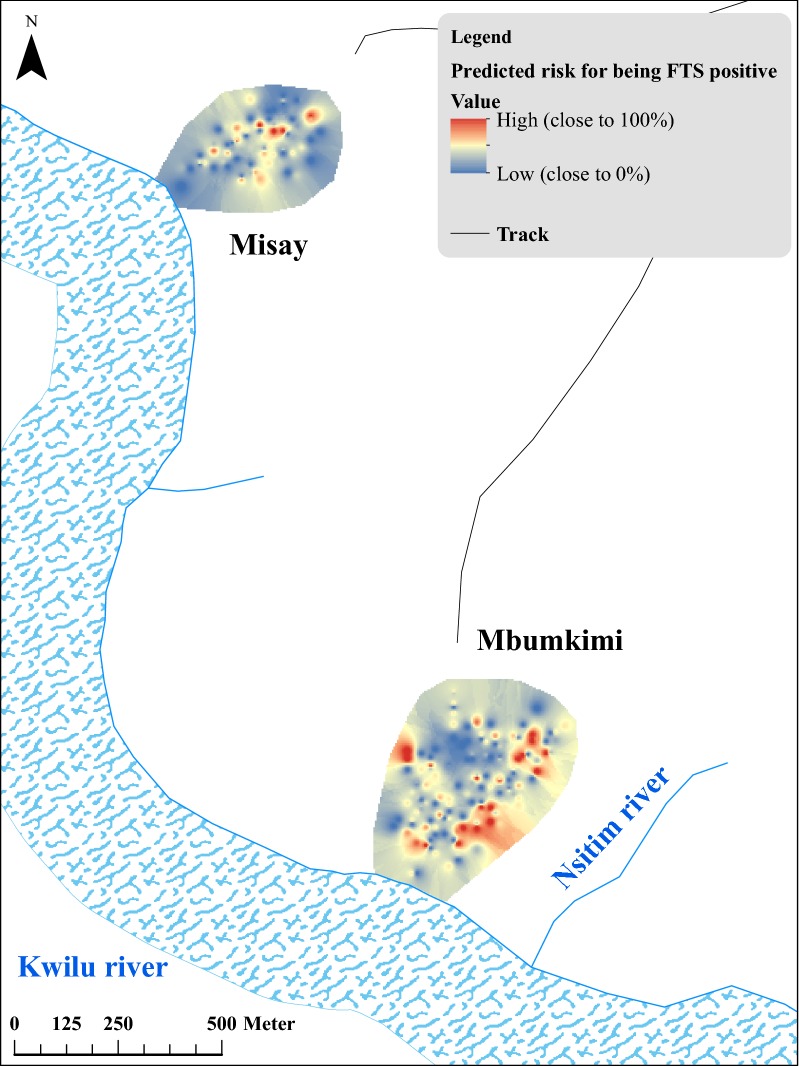
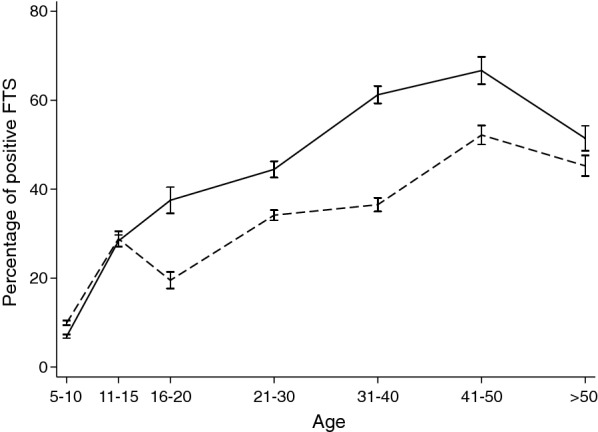
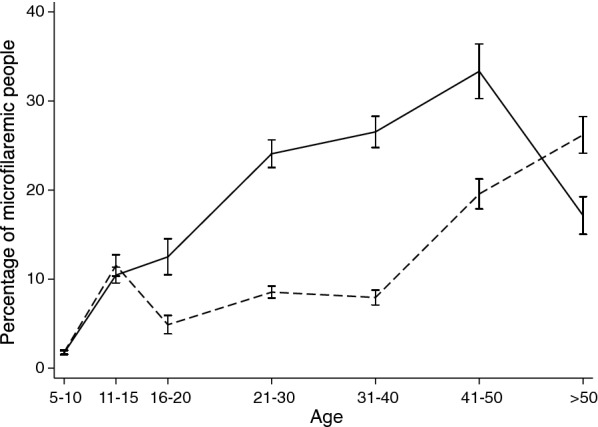
Two hundred and fifty nine out of 820 (31.6%) of subjects aged ≥ 5 years had W. bancrofti antigenaemia and 11.8% (97/820) had microfilaraemia. Multivariable analysis of risk factors for antigenaemia demonstrated increased risk for males (aOR = 1.75, 95% CI: 1.20-2.53, P = 0.003), for older individuals (aOR = 9.12 in those aged > 35 years, 95% CI: 4.47-18.61, P < 0.001), for people not using bednets (aOR = 1.57, 95% CI: 1.06-2.33, P = 0.023), for farmers (aOR = 2.21, 95% CI: 1.25-3.90, P = 0.006), and for those who live close to a river (aOR = 2.78, 95% CI: 1.14-6.74, P = 0.024). Significant risk factors for microfilaraemia included age, male gender, overnight stay in the bush, and residence close to a river (aOR = 1.86, 2.01, 2.73; P = 0.011, 0.010, 0.041; for the three latter variables, respectively). People who reported having taken levamisole (n = 117) during the prior year had a significantly decreased risk of having filarial antigenaemia (aOR = 0.40, 95% CI: 0.21-0.76, P = 0.005).
Age, sex, not using bednets, and occupation-dependent exposure to mosquitoes were important risk factors for infection with W. bancrofti in this study. The association with levamisole use suggests that the drug may have prevented filarial infections. Other results suggest that transmission often occurs outside of the village. This study provides interesting clues regarding the epidemiology of LF in Central Africa.
人们对中非国家淋巴丝虫病(LF)的风险因素知之甚少。为了进一步了解这方面的知识,我们研究了刚果民主共和国两个流行地区的 LF 流行病学。
依赖变量是用丝虫检测带(FTS)检测到的班氏吴策线虫抗原血症和夜间血涂片检测到的微丝蚴血症。研究了以下因素:性别、年龄、使用蚊帐、使用厕所、狩猎、捕鱼和农业活动、使用驱虫药治疗史、在灌木丛中过夜、人口密度、家庭人口数以及与河流的距离。采用混合多元逻辑回归模型进行分析。
820 名年龄≥5 岁的受试者中有 259 人(31.6%)存在班氏吴策线虫抗原血症,11.8%(97/820)存在微丝蚴血症。对感染因素进行多变量分析显示,男性(优势比[OR]为 1.75,95%可信区间:1.20-2.53,P=0.003)、年龄较大(年龄>35 岁的 OR 为 9.12,95%可信区间:4.47-18.61,P<0.001)、不使用蚊帐(OR 为 1.57,95%可信区间:1.06-2.33,P=0.023)、农民(OR 为 2.21,95%可信区间:1.25-3.90,P=0.006)和居住在河流附近(OR 为 2.78,95%可信区间:1.14-6.74,P=0.024)的人群感染风险增加。微丝蚴血症的显著危险因素包括年龄、男性、在灌木丛中过夜和靠近河流居住(OR 分别为 1.86、2.01、2.73;P=0.011、0.010、0.041)。在过去一年中报告服用左旋咪唑(n=117)的人群感染班氏吴策线虫的抗原血症风险显著降低(OR 为 0.40,95%可信区间:0.21-0.76,P=0.005)。
在这项研究中,年龄、性别、不使用蚊帐和与蚊子接触有关的职业是感染班氏吴策线虫的重要危险因素。与左旋咪唑使用的关联表明,该药物可能预防了丝虫感染。其他结果表明,传播经常发生在村庄之外。本研究为中非淋巴丝虫病的流行病学提供了有趣的线索。