Martinage Geoffrey, Geffrelot Julien, Stefan Dinu, Bogart Emilie, Rault Erwan, Reyns Nicolas, Emery Evelyne, Makhloufi-Martinage Samira, Mouttet-Audouard Raphaelle, Basson Laurent, Mirabel Xavier, Lartigau Eric, Pasquier David
Academic Department of Radiation Oncology, Centre Oscar Lambret, University Lille II, Lille, France.
Department of Radiation Oncology, Centre François Baclesse, Caen, France.
Front Oncol. 2019 Mar 28;9:184. doi: 10.3389/fonc.2019.00184. eCollection 2019.
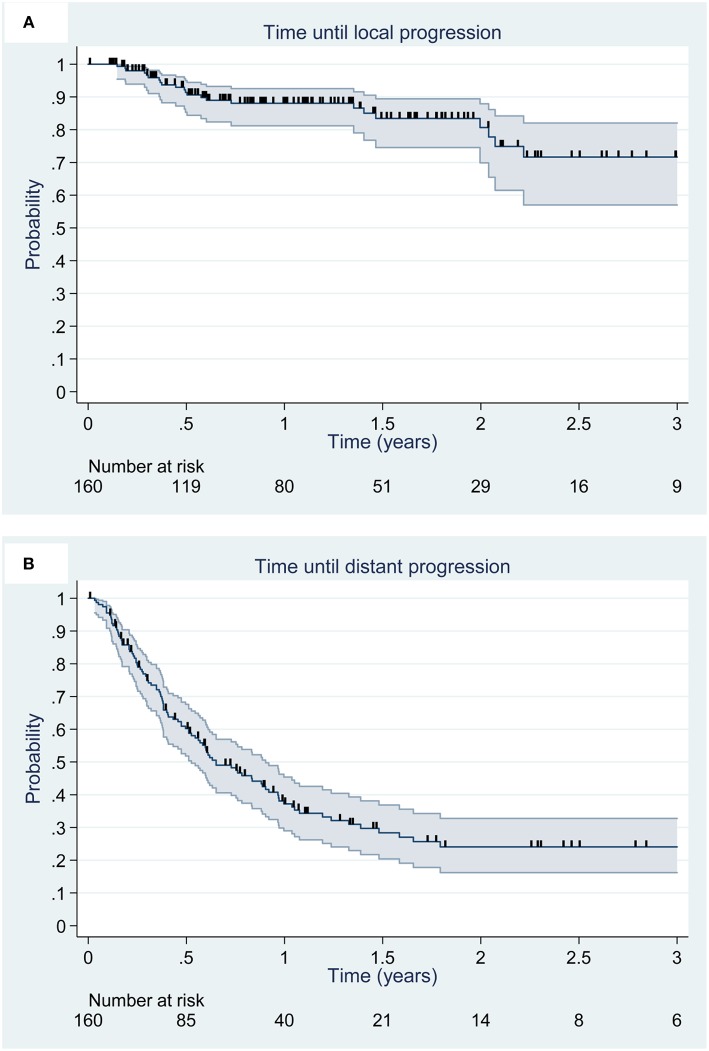
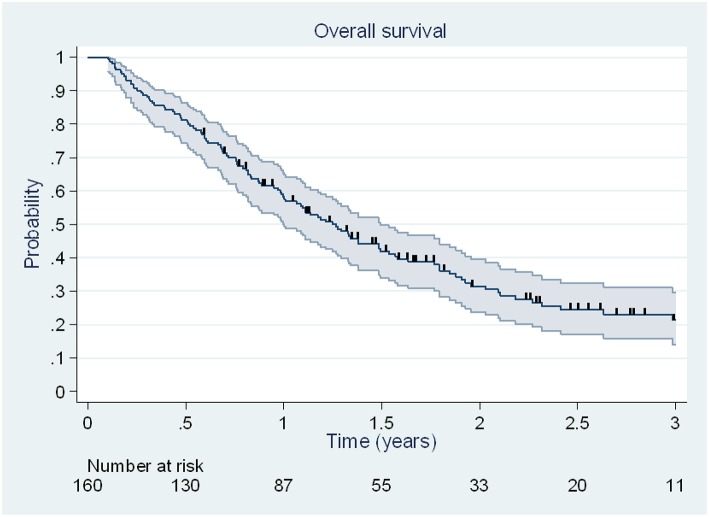
The aim of this study was to assess, in a large series, the efficacy and tolerance of post-operative adjuvant hypofractionated stereotactic radiation therapy (HFSRT) for brain metastases (BMs). Between July 2012 and January 2017, 160 patients from 2 centers were operated for BM and treated by HFSRT. Patients had between 1 and 3 BMs, no brainstem lesions or carcinomatous meningitis. The primary endpoint was local control. Secondary endpoints were distant brain control, overall survival (OS) and tolerance to HFSRT. 73 patients (46%) presented with non-small cell lung cancer (NSCLC), 23 (14%) had melanoma and 21 (13%) breast cancer. Median age was 58 years (range, 22-83 years). BMs were synchronous in 50% of the cases. The most frequent prescription regimens were 24 Gy in 3 fractions ( = 52, 33%) and 30 Gy in 5 fractions ( = 37, 23%). Local control rates at 1 and 2 years were 88% [95%CI, 81-93%] and 81% [95%CI, 70-88%], respectively. Distant control rate at 1 year was 48% [95%CI, 81-93%]. In multivariate analysis, primary NSCLC was associated with a significant reduction in the risk of death compared to other primary sites (HR = 0.57, = 0.007), the number of extra-cerebral metastatic sites (HR = 1.26, = 0.003) and planning target volumes (HR = 1.15, = 0.012) were associated with a lower OS. There was no prognostic factor of time to local progression. Median OS was 15.2 months [95%CI, 12.0-17.9 months] and the OS rate at 1 year was 58% [95% CI, 50-65%]. Salvage radiotherapy was administered to 72 patients (45%), of which 49 received new HFSRT. Ten (7%) patients presented late grade 2 and 4 (3%) patients late grade 3 toxicities. Thirteen (8.9%) patients developed radiation necrosis. This large multicenter retrospective study shows that HFSRT allows for good local control of metastasectomy tumor beds and that this technique is well-tolerated by patients.
本研究旨在评估在大量病例中,术后辅助超分割立体定向放射治疗(HFSRT)对脑转移瘤(BMs)的疗效和耐受性。2012年7月至2017年1月期间,来自2个中心的160例患者接受了BM手术并接受了HFSRT治疗。患者有1至3个BMs,无脑干病变或癌性脑膜炎。主要终点是局部控制。次要终点是远处脑控制、总生存期(OS)和对HFSRT的耐受性。73例(46%)患者为非小细胞肺癌(NSCLC),23例(14%)为黑色素瘤,21例(13%)为乳腺癌。中位年龄为58岁(范围22 - 83岁)。50%的病例中BMs为同步性。最常用的处方方案是3次分割24 Gy(n = 52,33%)和5次分割30 Gy(n = 37,23%)。1年和2年的局部控制率分别为88%[95%CI,81 - 93%]和81%[95%CI,70 - 88%]。1年的远处控制率为48%[95%CI,81 - 93%]。多因素分析显示,与其他原发部位相比,原发性NSCLC与死亡风险显著降低相关(HR = 0.57,P = 0.007),脑外转移部位数量(HR = 1.26,P = 0.003)和计划靶体积(HR = 1.15,P = 0.012)与较低的OS相关。没有局部进展时间的预后因素。中位OS为15.2个月[95%CI,12.0 - 17.9个月],1年的OS率为58%[95%CI,50 - 65%]。72例(45%)患者接受了挽救性放疗,其中49例接受了新的HFSRT。10例(7%)患者出现晚期2级毒性反应,4例(3%)患者出现晚期3级毒性反应。13例(8.9%)患者发生放射性坏死。这项大型多中心回顾性研究表明,HFSRT能实现对转移瘤切除瘤床的良好局部控制,且该技术患者耐受性良好。