Section of Rheumatology and Clinical Immunology, Department of General Internal Medicine, The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
Department of Rheumatology and Rehabilitation, Faculty of Medicine, Assiut University Hospitals, Assiut, Egypt.
J Immunother Cancer. 2019 Apr 16;7(1):106. doi: 10.1186/s40425-019-0585-1.
Checkpoint inhibitors (CPIs) have revolutionized the treatment of cancer, but their use remains limited by off-target inflammatory and immune-related adverse events. Solid organ transplantation (SOT) recipients have been excluded from clinical trials owing to concerns about alloimmunity, organ rejection, and immunosuppressive therapy. Thus, we conducted a retrospective study and literature review to evaluate the safety of CPIs in patients with cancer and prior SOT.
Data were collected from the medical records of patients with cancer and prior SOT who received CPIs at The University of Texas MD Anderson Cancer Center from January 1, 2004, through March 31, 2018. Additionally, we systematically reviewed five databases through April 2018 to identify studies reporting CPIs to treat cancer in SOT recipients. We evaluated the safety of CPIs in terms of alloimmunity, immune-related adverse events, and mortality. We also evaluated tumor response to CPIs.
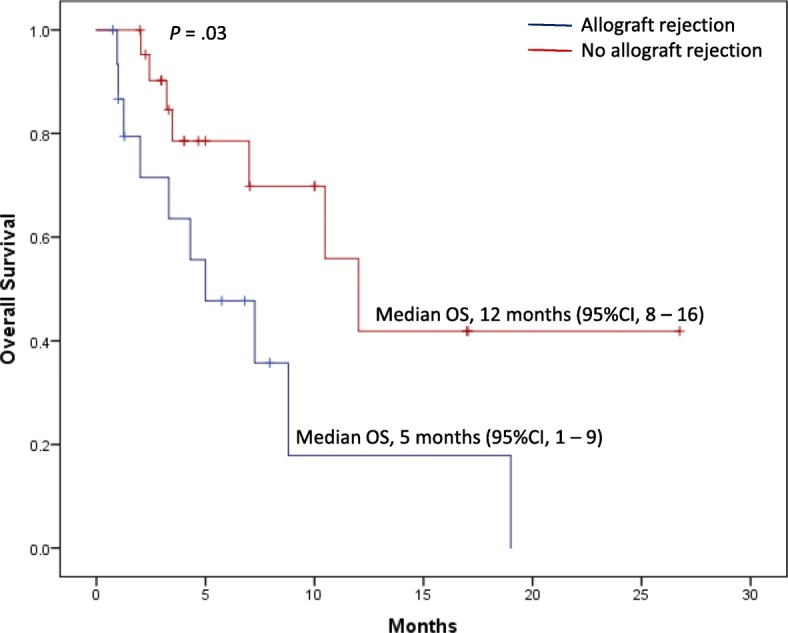
Thirty-nine patients with allograft transplantation were identified. The median age was 63 years (range 14-79 years), 74% were male, 62% had metastatic melanoma, 77% received anti-PD-1 agents, and 59% had prior renal transplantation, 28% hepatic transplantation, and 13% cardiac transplantation. Median time to CPI initiation after SOT was 9 years (range 0.92-32 years). Allograft rejection occurred in 41% of patients (11/23 renal, 4/11 hepatic, and 1/5 cardiac transplantations), at similar rates for anti-CTLA-4 and anti-PD-1 therapy. The median time to rejection was 21 days (95% confidence interval 19.3-22.8 days). There were no associations between time since SOT and frequency, timing, or type of rejection. Overall, 31% of patients permanently discontinued CPIs because of allograft rejection. Graft loss occurred in 81%, and death was reported in 46%. Of the 12 patients with transplantation biopsies, nine (75%) had acute rejection, and five of these rejections were T cell-mediated. In melanoma patients, 36% responded to CPIs.
SOT recipients had a high allograft rejection rate that was observed shortly after CPI initiation, with high mortality rates. Further studies are needed to optimize the anticancer treatment approach in these patients.
检查点抑制剂 (CPIs) 彻底改变了癌症的治疗方法,但由于对异体免疫、器官排斥和免疫抑制治疗的担忧,其应用仍然受到限制。由于担心异体免疫、器官排斥和免疫抑制治疗,实体器官移植 (SOT) 受者被排除在临床试验之外。因此,我们进行了一项回顾性研究和文献复习,以评估 CPI 在癌症和既往 SOT 患者中的安全性。
从 2004 年 1 月 1 日至 2018 年 3 月 31 日期间,在德克萨斯大学 MD 安德森癌症中心接受 CPI 治疗的癌症和既往 SOT 患者的病历中收集数据。此外,我们还通过 2018 年 4 月系统地审查了五个数据库,以确定报告 SOT 受者接受 CPI 治疗癌症的研究。我们从异体免疫、免疫相关不良事件和死亡率方面评估 CPI 的安全性。我们还评估了 CPI 对肿瘤的反应。
确定了 39 例同种异体移植患者。中位年龄为 63 岁(范围 14-79 岁),74%为男性,62%患有转移性黑色素瘤,77%接受了抗 PD-1 药物治疗,59%有既往肾移植、28%有肝移植和 13%有心脏移植。SOT 后开始 CPI 治疗的中位时间为 9 年(范围 0.92-32 年)。41%的患者发生同种异体排斥(23 例肾移植中有 11 例,11 例肝移植中有 4 例,5 例心脏移植中有 1 例),抗 CTLA-4 和抗 PD-1 治疗的发生率相似。排斥反应的中位时间为 21 天(95%置信区间为 19.3-22.8 天)。SOT 后时间与排斥的频率、时间或类型均无关联。总体而言,由于同种异体排斥,31%的患者永久停止了 CPI 治疗。移植物丢失率为 81%,死亡率为 46%。在 12 例接受移植活检的患者中,9 例(75%)发生急性排斥反应,其中 5 例为 T 细胞介导的排斥反应。在黑色素瘤患者中,36%对 CPI 有反应。
SOT 受者的同种异体移植排斥率很高,在 CPI 治疗开始后不久即可观察到,死亡率也很高。需要进一步研究以优化这些患者的抗癌治疗方法。