From Amsterdam UMC (J.A.N.B., L.J.B., A.P.), Vrije Universiteit Amsterdam, Department of Neurology, MS Center and Neuro-ophthalmology Expertise Center, Neuroscience Amsterdam; Amsterdam UMC (J.A.N.B., L.J.v.R., H.S.T., A.P.), Vrije Universiteit Amsterdam, Department of Ophthalmology, Neuro-ophthalmology Expertise Center, Neuroscience Amsterdam; Onze Lieve Vrouwe Gasthuis (L.J.v.R., B.M.J.U.), Department of Ophthalmology, Amsterdam, the Netherlands; and Moorfields Eye Hospital and the National Hospital for Neurology and Neurosurgery (A.P.), London, UK.
Neurology. 2019 May 14;92(20):e2299-e2308. doi: 10.1212/WNL.0000000000007499. Epub 2019 Apr 19.
We present an objective and quantitative approach for diagnosing internuclear ophthalmoplegia (INO) in multiple sclerosis (MS).
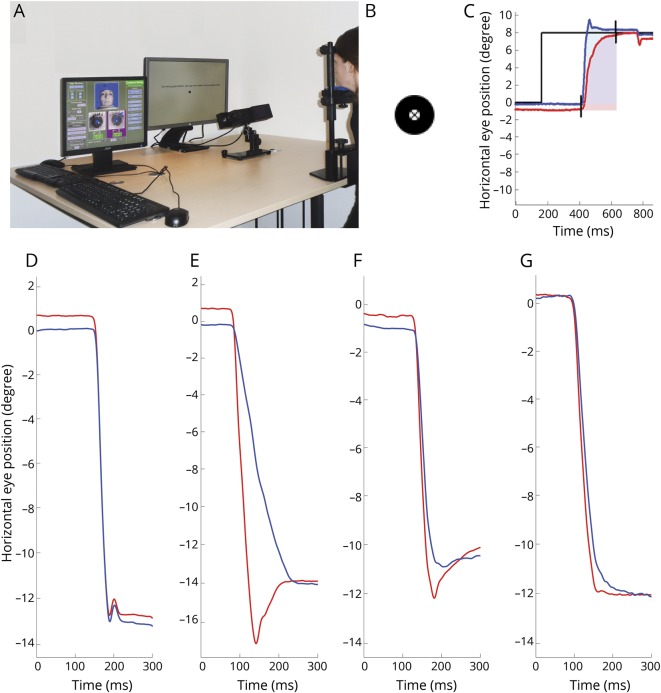
A validated standardized infrared oculography protocol (DEMoNS [Demonstrate Eye Movement Networks with Saccades]) was used for quantifying prosaccades in patients with MS and healthy controls (HCs). The versional dysconjugacy index (VDI) was calculated, which describes the ratio between the abducting and adducting eye. The VDI was determined for peak velocity, peak acceleration, peak velocity divided by amplitude, and area under the curve (AUC) of the saccadic trajectory. We calculated the diagnostic accuracy for the several VDI parameters by a receiver operating characteristic analysis comparing HCs and patients with MS. The National Eye Institute Visual Function Questionnaire-25 was used to investigate vision-related quality of life of MS patients with INO.
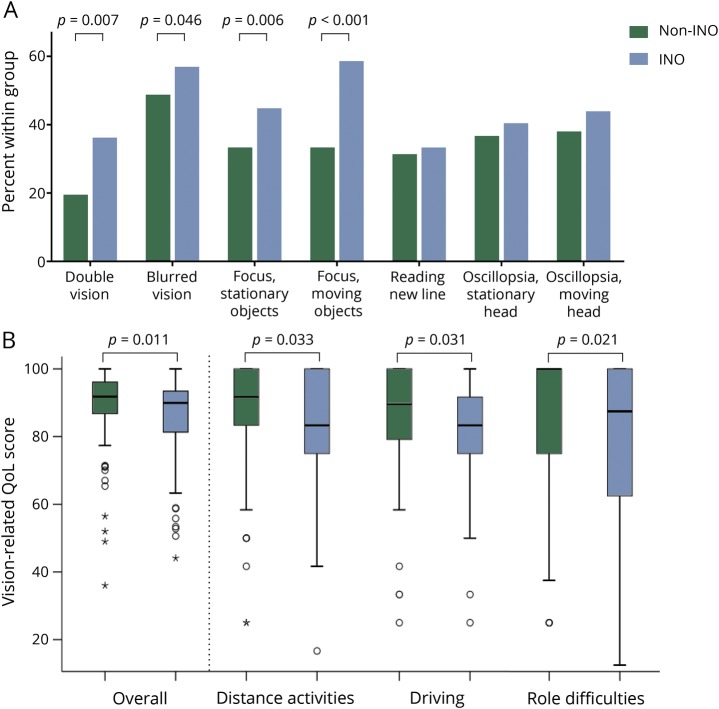
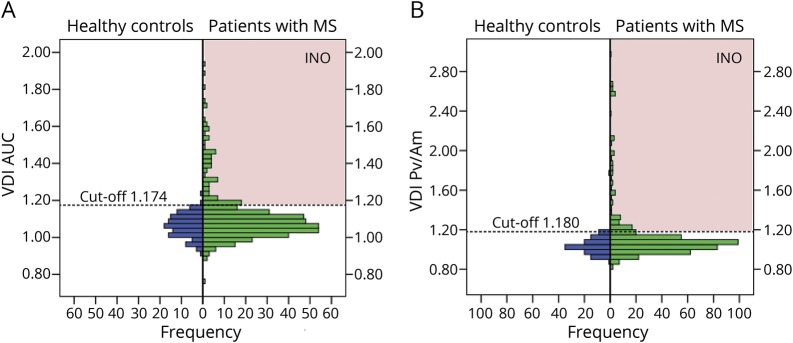
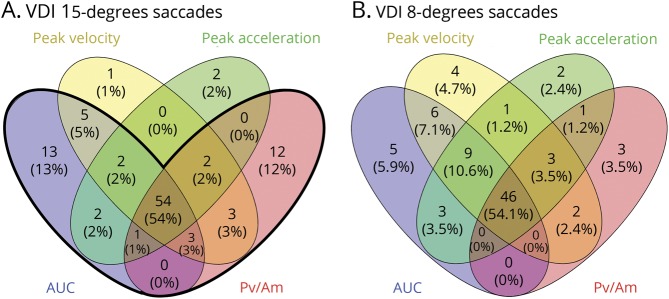
Two hundred ten patients with MS and 58 HCs were included. The highest diagnostic accuracy was achieved by the VDI AUC of 15° horizontal prosaccades. Based on a combined VDI AUC and peak velocity divided by amplitude detection, the prevalence of an INO in MS calculated to 34%. In the INO group, 35.2% of the patients with MS reported any complaints of double vision, compared to 18.4% in the non-INO group ( = 0.010). MS patients with an INO had a lower overall vision-related quality of life (median 89.9, interquartile range 12.8) compared to patients without an INO (median 91.8, interquartile range 9.3, = 0.011).
This study provides an accurate quantitative and clinically relevant definition of an INO in MS. This infrared oculography-based INO standard will require prospective validation. The high prevalence of INO in MS provides an anatomically well described and accurately quantifiable model for treatment trials in MS.
我们提出了一种客观、定量的方法来诊断多发性硬化症(MS)中的核间性眼肌麻痹(INO)。
使用经过验证的标准化红外眼动记录协议(DEMoNS [用扫视演示眼球运动网络])来量化 MS 患者和健康对照者(HCs)的正发性扫视。计算偏斜性失共轭指数(VDI),该指数描述了外展和内收眼之间的比值。VDI 是根据扫视轨迹的峰值速度、峰值加速度、峰值速度除以振幅和曲线下面积(AUC)来确定的。我们通过比较 HCs 和 MS 患者的受试者工作特征分析来计算几个 VDI 参数的诊断准确性。使用国家眼科研究所视觉功能问卷-25 来调查 INO 多发性硬化症患者的视力相关生活质量。
共纳入 210 名 MS 患者和 58 名 HCs。水平 15°正发性扫视的 VDI AUC 具有最高的诊断准确性。基于 VDI AUC 和峰值速度除以振幅的联合检测,MS 患者中 INO 的患病率计算为 34%。在 INO 组中,35.2%的 MS 患者报告有任何复视症状,而非 INO 组为 18.4%( = 0.010)。存在 INO 的 MS 患者的整体视力相关生活质量(中位数 89.9,四分位距 12.8)低于无 INO 的患者(中位数 91.8,四分位距 9.3, = 0.011)。
本研究提供了一种准确的定量和具有临床相关性的 MS 中 INO 定义。这种基于红外眼动记录的 INO 标准需要前瞻性验证。MS 中 INO 的高患病率为 MS 的治疗试验提供了一种解剖学上描述良好且可准确量化的模型。