Li Weichao, Sun Xianrun, Li Hongrong, Meng Zengdong, Yang Yong, Yao Shaoping
Faculty of Medical Science, Kunming University of Science and Technology.
Department of Orthopedic Surgery.
Medicine (Baltimore). 2019 Apr;98(16):e15306. doi: 10.1097/MD.0000000000015306.
The coexistence of a tuberculous aortic pseudoaneurysm and Pott disease in patients with a history of tuberculosis (TB) is relatively rare, and the treatment strategies remain still controversial.
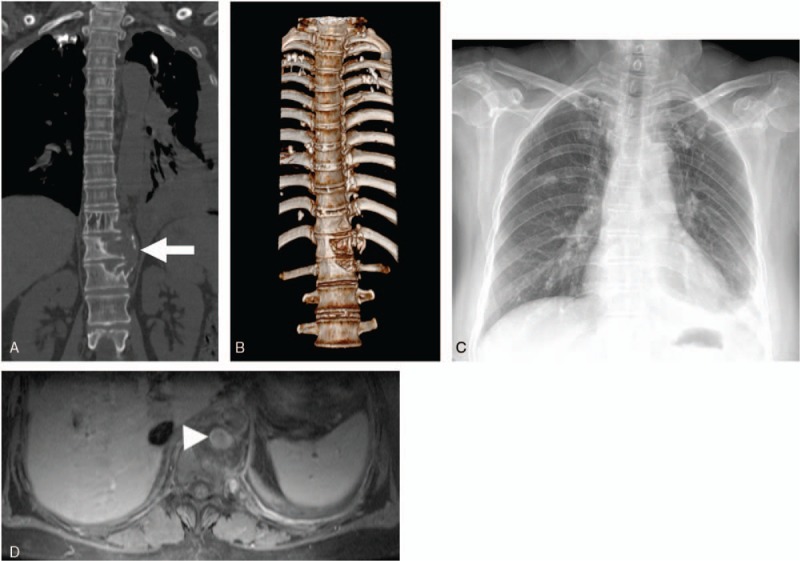
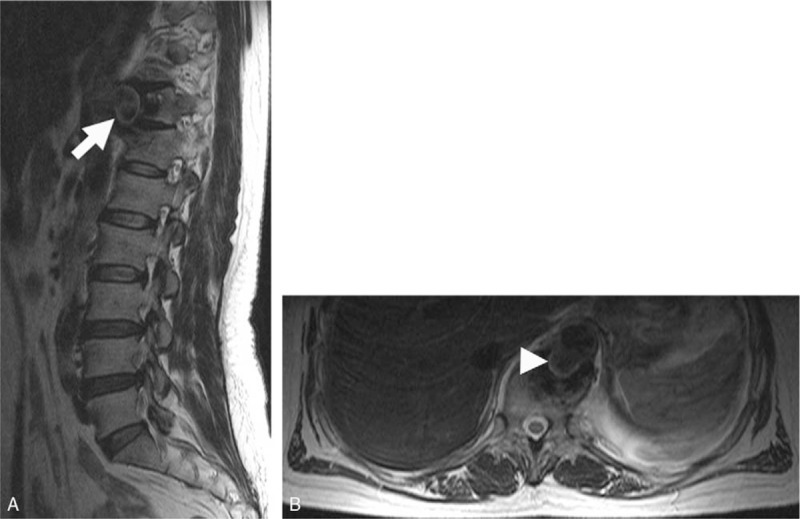
A 57-year-old female patient with a history of primary pulmonary TB presented with symptoms of breathlessness, chest pain, weight loss, and fever. Magnetic resonance imaging (MRI) and computed tomography (CT) showed a thoracic aortic pseudoaneurysm secondary to Pott disease at T11/12 level.
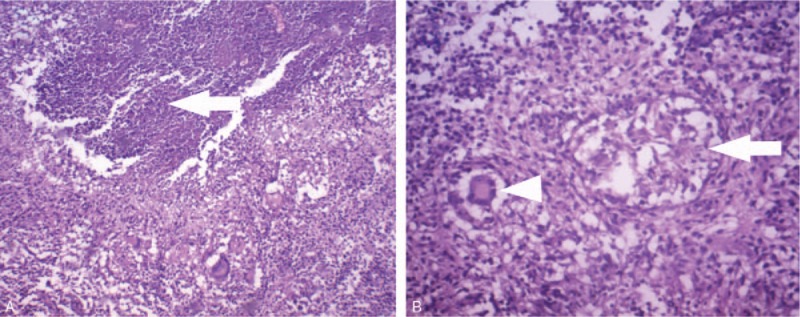
Tuberculous pseudoaneurysm at the descending thoracic aorta associated with tuberculous vertebral osteomyelitis.
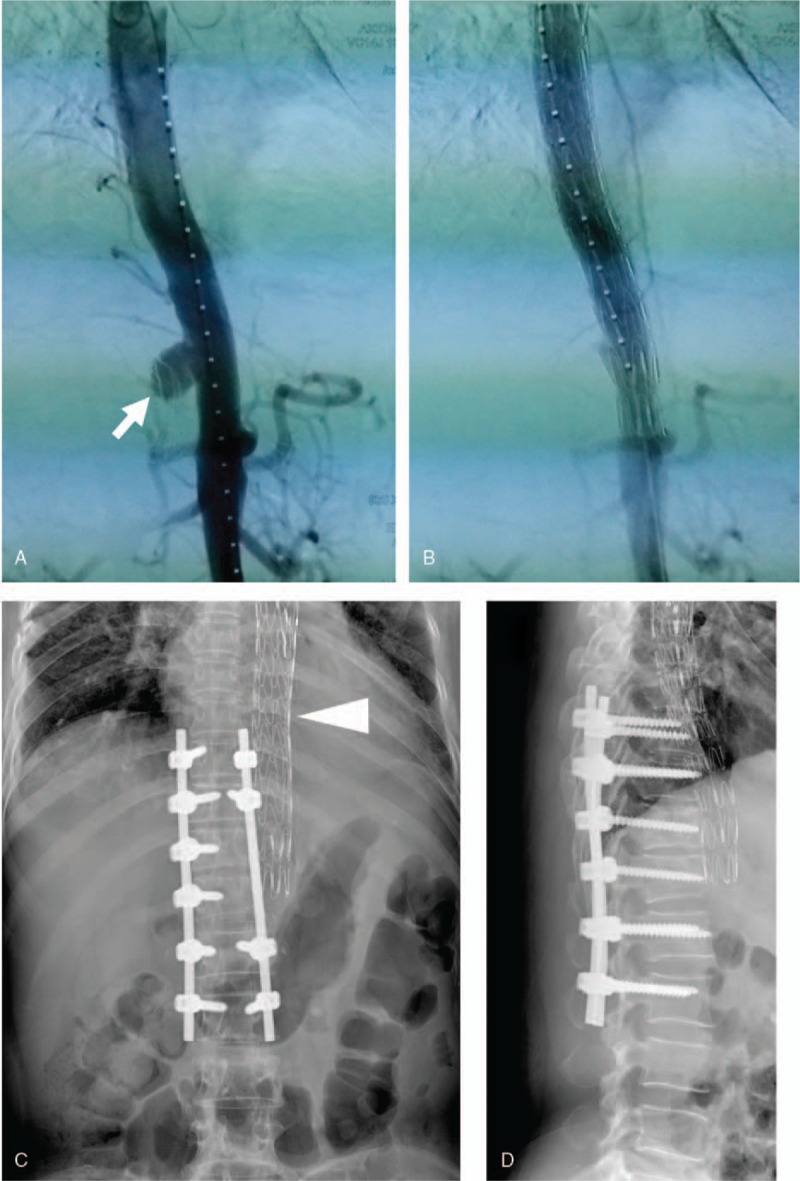
We originally planned a combined surgery consisting of posterior spine stabilization, anterior excision of the infected field, and aortic reconstruction. When we surgically stabilized the posterior spine, unexpectedly, the pseudoaneurysm ruptured. Immediately, we terminated the surgery and appropriately placed an endovascular stent graft, which successfully rescued the patient.
When the patient's conditions were stable, we anteriorly debrided all infected tissues and then performed a spinal fusion by grafting autologous iliac bone. After the debridement and spinal fusion, we arranged a 1-year anti-tuberculous chemotherapy for this patient and performed a 24-month follow-up. This patient had no signs of recurrent infection during the follow-up.
For the patients with tuberculous aortic aneurysm(s) complicated with vertebral osteomyelitis, the endovascular repair of an aneurysm(s) should be considered a conventional therapy before the spine surgery, lowering the risk of aortic aneurysm rupture. Meanwhile, minimally invasive endovascular stent graft combined with anti-tuberculosis drugs may be considered one of the therapeutic regimens for the patients whose conditions are not suitable for open surgery, such as age, weakness, or severe organ failure.
有结核病史的患者中,结核性主动脉假性动脉瘤与波特病并存相对少见,治疗策略仍存在争议。
一名57岁有原发性肺结核病史的女性患者,出现呼吸困难、胸痛、体重减轻和发热症状。磁共振成像(MRI)和计算机断层扫描(CT)显示在T11/12水平因波特病继发胸主动脉假性动脉瘤。
降主动脉结核性假性动脉瘤合并结核性椎体骨髓炎。
我们最初计划进行联合手术,包括后路脊柱稳定术、感染灶前路切除和主动脉重建。当我们手术稳定后路脊柱时,意外的是假性动脉瘤破裂。我们立即终止手术并合适地置入血管内支架移植物,成功挽救了患者。
当患者病情稳定后,我们前路清创所有感染组织,然后通过自体髂骨移植进行脊柱融合。清创和脊柱融合后,我们为该患者安排了为期1年的抗结核化疗并进行了24个月的随访。该患者在随访期间无反复感染迹象。
对于合并椎体骨髓炎的结核性主动脉瘤患者,在脊柱手术前应将动脉瘤的血管内修复视为常规治疗,降低主动脉瘤破裂风险。同时,对于因年龄、虚弱或严重器官衰竭等不适合开放手术的患者,微创血管内支架移植物联合抗结核药物可被视为治疗方案之一。