Committee of Renal Data Registry, Japanese Society for Dialysis Therapy, Tokyo, Japan.
Committee of Renal Data Registry, Japanese Society for Dialysis Therapy, Tokyo, Japan
J Am Soc Nephrol. 2019 Jun;30(6):1037-1048. doi: 10.1681/ASN.2018101007. Epub 2019 Apr 23.
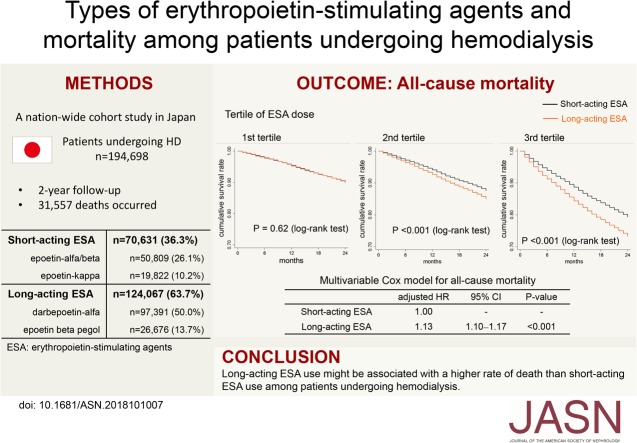
Despite the widespread use of erythropoietin-stimulating agents (ESAs) to treat anemia in patients undergoing hemodialysis, the relative mortality risks associated with use of different types of ESAs are unknown.
To compare the mortality risk associated with use of short-acting ESAs versus long-acting ESAs, we conducted a nationwide cohort study of 194,698 hemodialysis patients in Japan who received either a short-acting (epoetin / or epoetin ) or a long-acting (darbepoetin or epoetin β pegol) ESA. Study outcomes were 2-year all-cause and cause-specific mortality. In addition to Cox proportional hazards models, we performed an instrumental variable analysis in which facility-level long-acting ESA prescription rates were taken as the instrumental variable.
During the 2-year follow-up period, 31,557 deaths occurred. In a multivariable Cox model, long-acting ESA users had a 13% higher rate of deaths compared with short-acting ESA users, a significant difference (<0.001). Similar results were obtained in other analyses. This difference in risk was pronounced among patients receiving high doses of ESA (for whom the adjusted 2-year number needed to harm for death was 30.8). Long-acting ESA use was associated with an increased rate of death from cardiovascular diseases, infection, and malignancies. In the instrumental variable analysis, long-acting ESA users remained at a significantly higher risk of death. Compared with anemic (hemoglobin 9.0-9.9 g/dl) short-acting ESA users, long-acting ESA users who achieved more optimal hemoglobin levels (10.0-10.9 g/dl) showed a higher mortality rate.
Among patients undergoing hemodialysis, use of long-acting ESAs might be associated with a higher risk of death than use of short-acting ESAs.
尽管促红细胞生成素刺激剂(ESAs)被广泛用于治疗血液透析患者的贫血,但不同类型 ESA 的使用与相对死亡率风险之间的关系尚不清楚。
为了比较使用短效 ESA 与长效 ESA 的死亡率风险,我们对日本 194698 名接受短效(促红素/或促红素)或长效(达贝泊汀或聚乙二醇化促红素β)ESA 的血液透析患者进行了一项全国性队列研究。研究结局为 2 年全因死亡率和死因特异性死亡率。除了 Cox 比例风险模型外,我们还进行了工具变量分析,其中将机构层面的长效 ESA 处方率作为工具变量。
在 2 年的随访期间,有 31557 例死亡。在多变量 Cox 模型中,长效 ESA 使用者的死亡率比短效 ESA 使用者高 13%,差异有统计学意义(<0.001)。其他分析也得到了类似的结果。在接受高剂量 ESA 的患者中(需要治疗 2 年的人数为 30.8 人),这种风险差异更为显著。长效 ESA 的使用与心血管疾病、感染和恶性肿瘤导致的死亡率增加有关。在工具变量分析中,长效 ESA 使用者的死亡风险仍然显著升高。与贫血(血红蛋白 9.0-9.9 g/dl)的短效 ESA 使用者相比,达到更理想血红蛋白水平(10.0-10.9 g/dl)的长效 ESA 使用者的死亡率更高。
在血液透析患者中,与使用短效 ESA 相比,使用长效 ESA 可能与更高的死亡风险相关。