Department of Rheumatology & Clinical Immunology, University Medical Center Utrecht, Utrecht University, G02.228, P.O. Box 85500, 3508GA, Utrecht, The Netherlands.
Curr Rheumatol Rep. 2019 Apr 23;21(6):24. doi: 10.1007/s11926-019-0821-1.
To review the effectiveness of remission induction strategies compared to single csDMARD-initiating strategies according to current guidelines in early RA.
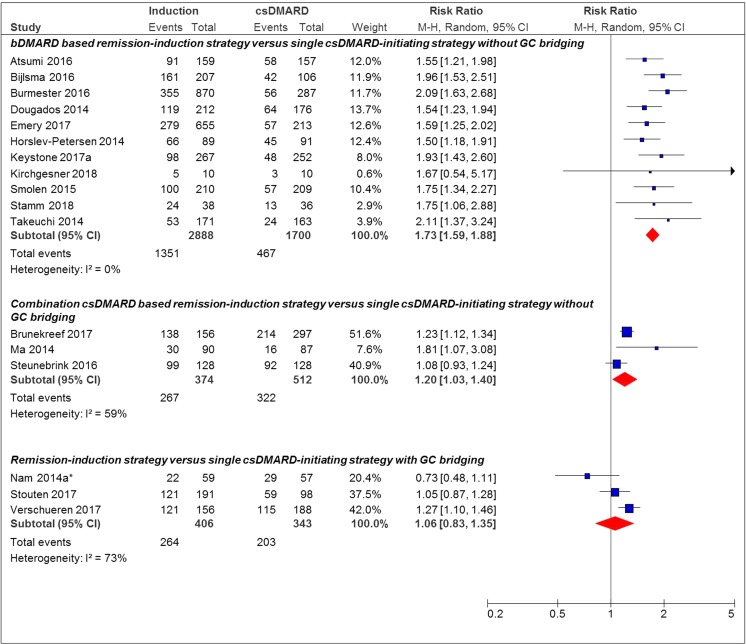
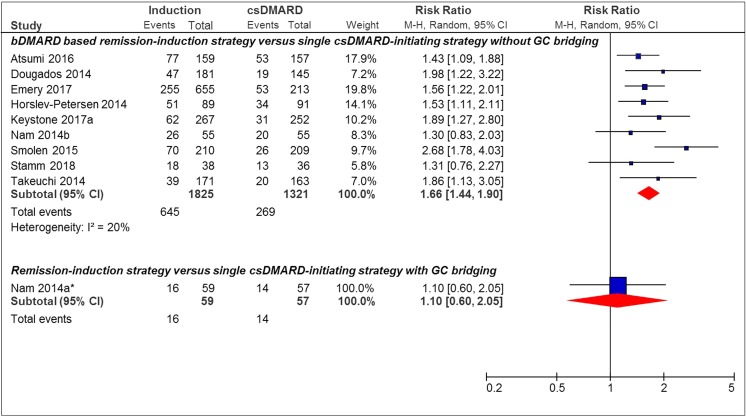
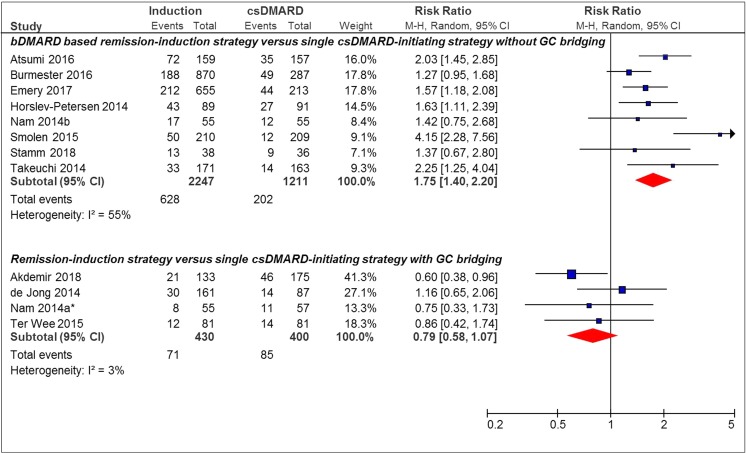
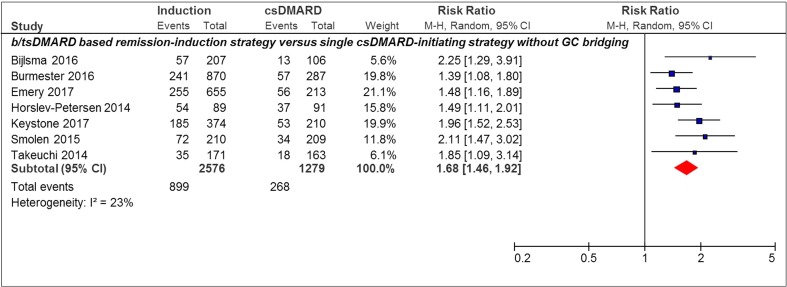
Twenty-nine studies, heterogeneous on, e.g., specific treatment strategy and remission outcome used, were identified. Using DAS28-remission over 12 months, 13 (76%) of 17 remission induction strategies showed significantly more patients achieving remission. Pooled relative "risk" was 1.73 [95%CI 1.59-1.88] for bDMARD-based remission induction strategies and 1.20 [95%CI 1.03-1.40] for combination csDMARD-based remission induction strategies compared to single csDMARD-initiating strategies. When additional glucocorticoid "bridging therapy" was used in single csDMARD-initiating strategies, the higher proportion patients achieving remission in remission induction strategies was no longer statistically significant (pooled RR 1.06 [95%CI 0.83-1.35]). For other remission outcomes, results were in line with above. Remission induction strategies are more effective in achieving remission compared to single csDMARD-initiating strategies, possibly more so in bDMARD-based induction strategies. However, compared to single csDMARD-initiating strategies with glucocorticoids, induction strategies may not be more effective.
根据当前的指南,回顾在早期 RA 中,与单一 csDMARD 起始策略相比,缓解诱导策略的有效性。
确定了 29 项研究,这些研究在特定的治疗策略和缓解结果等方面存在异质性。使用 DAS28 缓解超过 12 个月,17 种缓解诱导策略中的 13 种(76%)显示出显著更多的患者达到缓解。基于生物制剂的缓解诱导策略的汇总相对“风险”为 1.73[95%CI 1.59-1.88],联合 csDMARD 基于缓解诱导策略的汇总相对“风险”为 1.20[95%CI 1.03-1.40],与单一 csDMARD 起始策略相比。当在单一 csDMARD 起始策略中使用额外的糖皮质激素“桥接治疗”时,缓解诱导策略中达到缓解的患者比例不再具有统计学意义(汇总 RR 1.06[95%CI 0.83-1.35])。对于其他缓解结果,结果与上述结果一致。与单一 csDMARD 起始策略相比,缓解诱导策略在达到缓解方面更有效,基于生物制剂的诱导策略可能更有效。然而,与具有糖皮质激素的单一 csDMARD 起始策略相比,诱导策略可能并不更有效。