Department of Diagnostic and Interventional Radiology, University of Leipzig, Leipzig, Germany.
Department of Surgery, Campus Virchow and Campus Mitte, Charité - Universitätsmedizin Berlin, Berlin, Germany.
BMC Med Imaging. 2019 Apr 27;19(1):32. doi: 10.1186/s12880-019-0332-6.
The goal of our study was to evaluate the current approach in prediction of postoperative major complications after pancreaticoduodenectomy (PD), especially symptomatic pancreatic fistula (POPF), using parameters derived from computed tomography (CT).
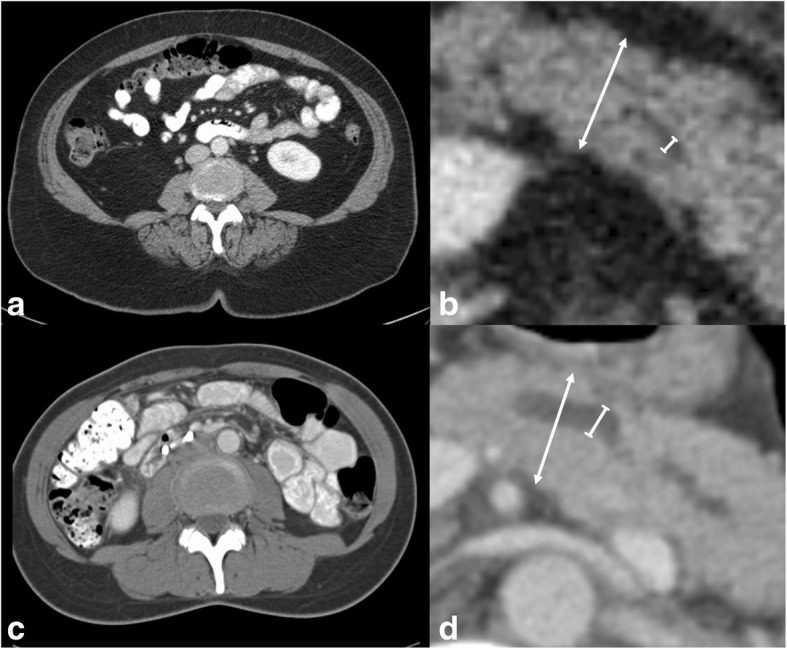
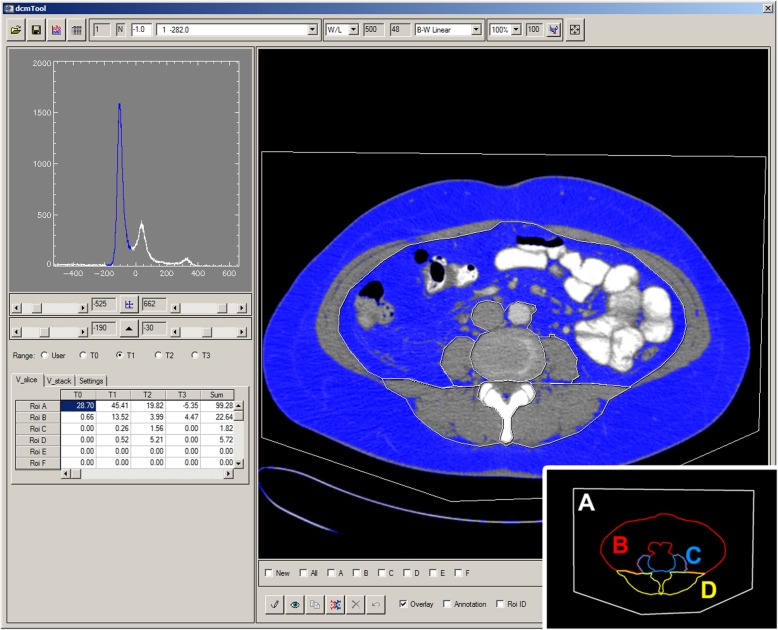
Patients after PD were prospectively collected in a database of the local department of surgery and all patients with CT scans available were assessed in this study. CT parameters were measured at the level of the intervertebral disc L3/L4 and consisted of the areas of the visceral adipose tissue (A), the diameters of the pancreatic parenchyma (DPP) and the pancreatic duct (DPD), the areas of ventral abdominal wall muscle (A), psoas muscle (A), paraspinal muscle (A), total muscle (A), as well as the mean muscle attenuation (MA) and skeletal muscle index (SMI). Mann-Whitney-U Test for two independent samples and binary logistic regression were used for statistical analysis.
One hundred thirty-nine patients (55 females, 84 males) were included. DPD was 2.9 mm (Range 0.7-10.7) on median and more narrow in patients with complications equal to or greater stadium IIIb (p < 0.04) and severe POPF (p < 0.01). DPP median value was 17 (6.9-37.9) mm and there was no significant difference regarding major complications or POPF. A showed a median value of 127.5 (14.5-473.0) cm and was significantly larger in patients with POPF (p < 0.01), but not in cases of major complications (p < 0.06). A, A, A and A showed no significant differences between major complications and POPF. MA was both lower in groups with major complications (p < 0.01) and POPF (p < 0.01). SMI failed to differentiate between patients with or without major complications or POPF.
Besides the known factors visceral obesity and narrowness of the pancreatic duct, the mean muscle attenuation can easily be examined on routine preoperative CT scans and seems to be promising parameter to predict postoperative complications and POPF.
我们的研究旨在评估目前使用计算机断层扫描(CT)得出的参数预测胰十二指肠切除术(PD)后主要术后并发症的方法,尤其是有症状的胰瘘(POPF)。
前瞻性收集当地外科部门的 PD 患者数据库,对所有有 CT 扫描的患者进行评估。在 L3/L4 椎间盘水平测量 CT 参数,包括内脏脂肪组织(A)、胰腺实质(DPP)和胰管(DPD)直径、腹前壁肌肉(A)、腰大肌(A)、脊柱旁肌肉(A)、总肌肉(A)、平均肌肉衰减(MA)和骨骼肌指数(SMI)。使用两独立样本的曼-惠特尼 U 检验和二项逻辑回归进行统计分析。
共纳入 139 例患者(女性 55 例,男性 84 例)。DPD 的中位数为 2.9mm(范围 0.7-10.7),并发症等于或大于 IIIb 期(p<0.04)和严重 POPF(p<0.01)的患者较狭窄。DPP 的中位数为 17mm(6.9-37.9),主要并发症或 POPF 之间无显著差异。A 的中位数为 127.5cm(14.5-473.0),POPF 患者明显更大(p<0.01),但主要并发症患者无显著差异(p<0.06)。A、A、A 和 A 之间在主要并发症和 POPF 之间无显著差异。MA 在有主要并发症的组(p<0.01)和 POPF 组(p<0.01)中均较低。SMI 未能区分有或无主要并发症或 POPF 的患者。
除了已知的因素内脏肥胖和胰管狭窄外,平均肌肉衰减在常规术前 CT 扫描中易于检查,似乎是预测术后并发症和 POPF 的有前途的参数。