Centre for Cancer Prevention, Wolfson Institute of Preventive Medicine, Queen Mary University of London, Charterhouse Square, London, EC1M 6BQ, UK.
Instituto de Investigacion Sanitaria Gregorio Marañon, CIBERONC, Universidad Complutense, Madrid, Spain.
Breast Cancer Res Treat. 2019 Jul;176(2):377-386. doi: 10.1007/s10549-019-05226-8. Epub 2019 Apr 30.
EndoPredict (EPclin) is a prognostic test validated to inform decisions on adjuvant chemotherapy to endocrine therapy alone for patients with oestrogen receptor-positive, HER2-negative breast cancer. Here, we determine the performance of EPclin for estimating 10-year distant recurrence-free interval (DRFI) rates for those who received adjuvant endocrine therapy (ET) alone compared to those with chemotherapy plus endocrine therapy (ET + C).
A total of 3746 women were included in this joint analysis. 2630 patients received 5 years of ET alone (ABCSG-6/8, TransATAC) and 1116 patients received ET + C (GEICAM 2003-02/9906). The primary objective was to evaluate the ability of EPclin to provide an estimate of the 10-year DR rate as a continuous function of EPclin separately for ET alone and ET + C. Cox proportional hazard models were used for these analyses.
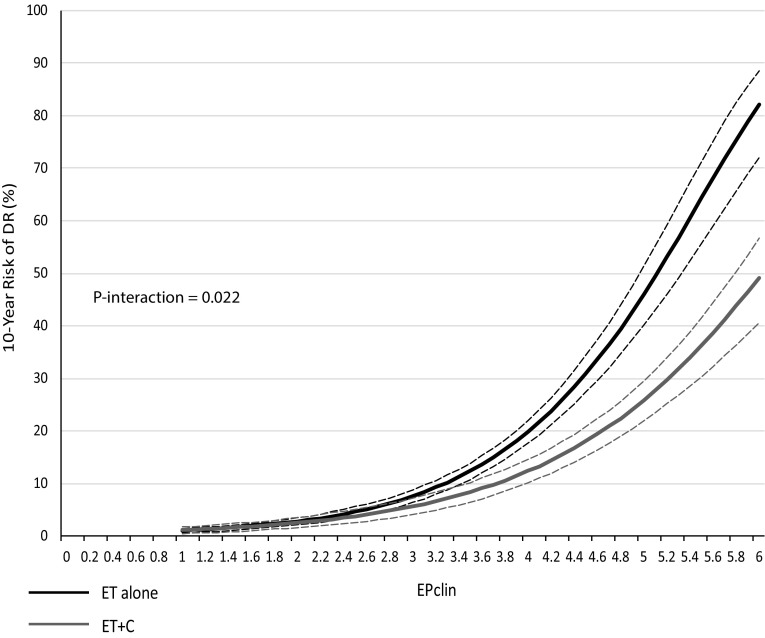
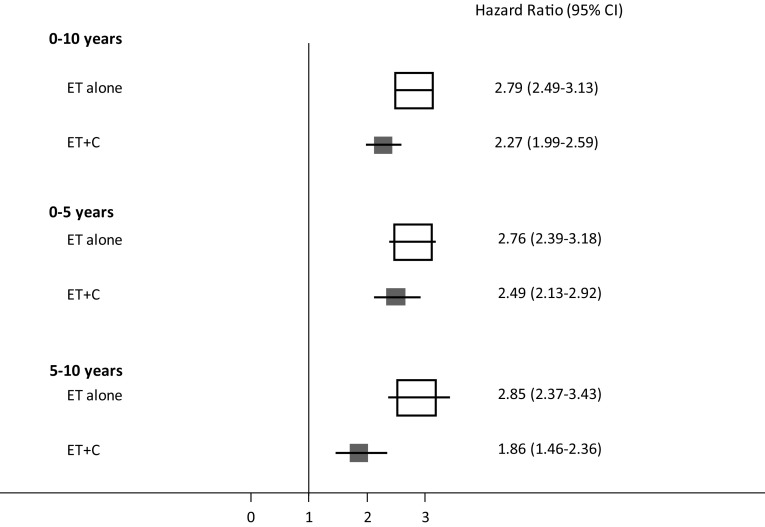
EPclin was highly prognostic for DR in women who received ET alone (HR 2.79 (2.49-3.13), P < 0.0001) as well as in those who received ET + C (HR 2.27 (1.99-2.59), P < 0.0001). Women who received ET + C had significantly smaller increases in 10-year DR rates with the increasing EPclin score than those receiving ET alone (EPclin = 5; 12% ET + C vs. 20% ET alone). We observed a significant positive interaction between EPclin and treatment groups (P- = 0.022).
In this comparative non-randomised analysis, the rate of increase in DR with EPclin score was significantly reduced in women who received ET + C versus ET alone. Our indirect comparisons suggest that a high EPclin score can predict chemotherapy benefit in women with ER-positive, HER2-negative disease.
EndoPredict(EPclin)是一种经过验证的预后测试,可用于指导激素受体阳性、HER2 阴性乳腺癌患者单独接受内分泌治疗与内分泌治疗联合化疗的决策。本研究旨在评估 EPclin 对单独接受辅助内分泌治疗(ET)与化疗联合内分泌治疗(ET+C)患者的 10 年远处无复发生存率(DRFI)的预测能力。
本联合分析共纳入 3746 例患者。2630 例患者接受 5 年 ET 单药治疗(ABCSG-6/8、TransATAC),1116 例患者接受 ET+C 治疗(GEICAM 2003-02/9906)。主要目的是评估 EPclin 分别在单独接受 ET 和 ET+C 治疗的患者中,作为连续函数预测 10 年 DR 率的能力。采用 Cox 比例风险模型进行这些分析。
EPclin 对单独接受 ET 治疗的患者(HR 2.79(2.49-3.13),P<0.0001)和接受 ET+C 治疗的患者(HR 2.27(1.99-2.59),P<0.0001)的 DR 均具有高度的预后价值。与单独接受 ET 治疗的患者相比,接受 ET+C 治疗的患者随着 EPclin 评分的升高,10 年 DR 率的增加幅度显著减小(EPclin=5;ET+C 组为 12%,ET 组为 20%)。我们观察到 EPclin 与治疗组之间存在显著的正交互作用(P=0.022)。
在这项非随机比较分析中,与单独接受 ET 治疗的患者相比,接受 ET+C 治疗的患者 EPclin 评分与 DR 增加之间的相关性显著减弱。我们的间接比较结果提示,高 EPclin 评分可预测 ER 阳性、HER2 阴性疾病患者的化疗获益。