Department of Obstetrics and Gynecology, School of Medicine, Technical University of Munich, Klinikum rechts der Isar, Munich, Germany.
Institute of Medical Informatics, Statistics and Epidemiology, School of Medicine, Technical University of Munich, Klinikum rechts der Isar, Munich, Germany.
Arch Gynecol Obstet. 2020 Dec;302(6):1461-1467. doi: 10.1007/s00404-020-05771-4. Epub 2020 Sep 9.
Prospectively collected outcome data of patients (pts) whose adjuvant systemic therapy recommendation was based on the clinico-molecular test EndoPredict (EP) are presented.
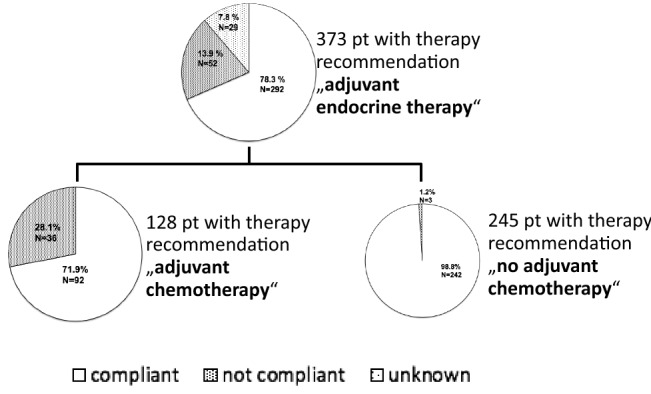
Pts with ER-positive, HER2-negative early breast cancer with 0-3 positive lymph nodes were enrolled. The EP was carried out on all tumor samples. Pts were evaluated for treatment compliance, local recurrence, distant metastases and overall survival. Censored time-to-event outcomes were analysed by Cox proportional hazards models. Additional estimates of the event-free-survival were calculated by the Kaplan-Meier method. Hypothesis testing was conducted on two-sided exploratory 5% significance levels.
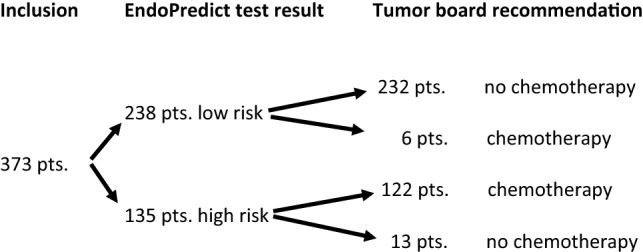
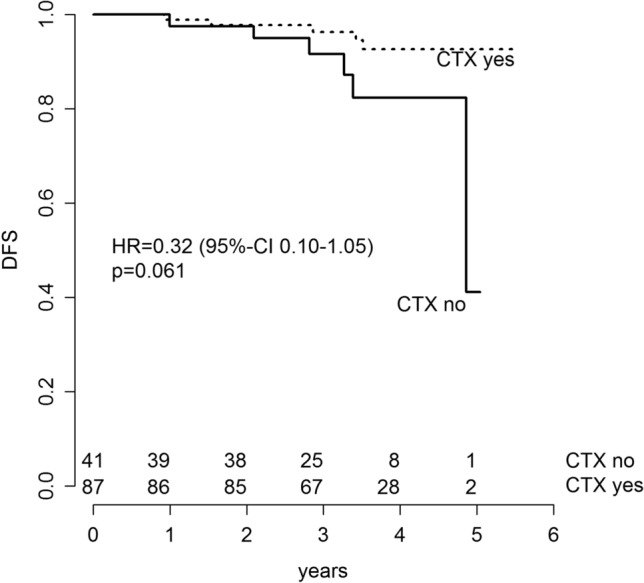
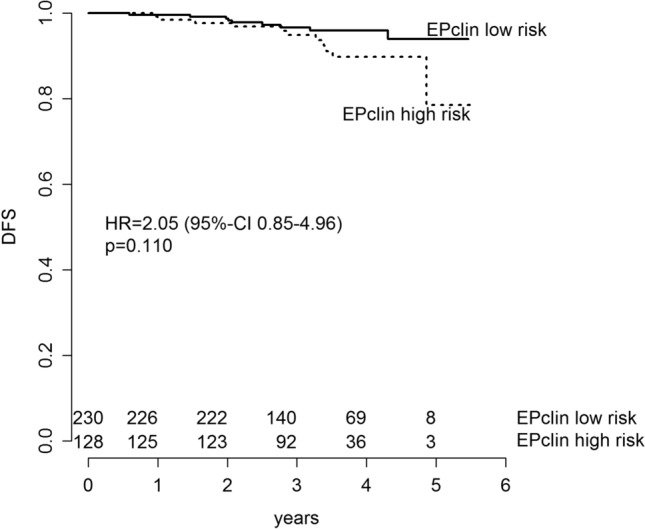
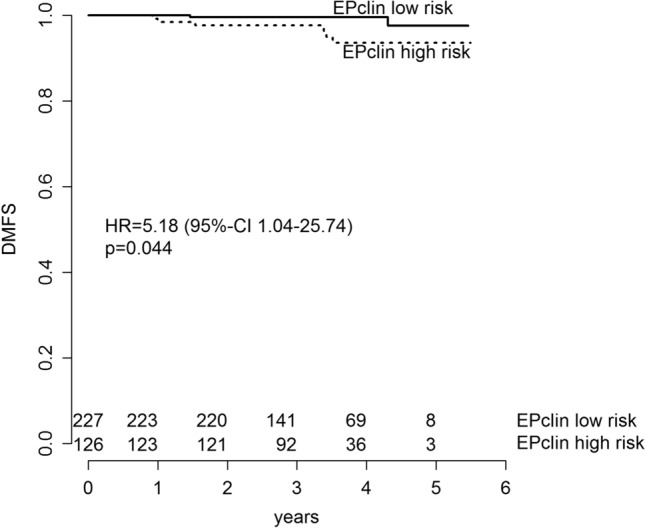
373 consecutive pts were enrolled. EP classified 238 pts (63.8%) as low risk and 135 pts (36.2%) as high risk. Median follow-up was 41.6 months. Risk for disease recurrence or death in EPclin high-risk patients was twofold higher in comparison with EPclin low-risk patients (hazard ratio (HR) 2.05 (95% CI 0.85-4.96; p = 0.110). Patients with EPclin high risk were at significant higher risk of distant metastases than patients with EPclin low risk (HR 5.18; 95% CI 1.04-25.74; p = 0.0443). EPclin high-risk patients who actually underwent adjuvant CTX had a 3-year-DFS of 96.3% (95% CI 92.2-100) in contrast to EPclin high-risk patients without CTX (3-year-DFS: 91.5% (95% CI 82.7-100%); HR 0.32; 95% CI 0.10-1.05; p = 0.061).
These first prospective outcome results show that EP, in clinical routine, is a valid clinico-molecular test, to predict DFS and to guide decision of adjuvant CTX use in ER-positive, HER2-negative early breast cancer pts with 0-3 positive lymph nodes. Adjuvant CTX seems to be beneficial for EPclin high-risk patients.
本文旨在前瞻性地收集基于临床分子检测 EndoPredict(EP)的辅助全身治疗建议的患者(pts)的结局数据。
纳入了 ER 阳性、HER2 阴性、淋巴结 0-3 阳性的早期乳腺癌患者。所有肿瘤样本均进行 EP 检测。评估 pts 的治疗依从性、局部复发、远处转移和总生存情况。使用 Cox 比例风险模型分析censored 时间事件结局。通过 Kaplan-Meier 方法计算无事件生存的额外估计值。采用双侧探索性 5%显著性水平进行假设检验。
共纳入 373 例连续 pts。EP 将 238 例 pts(63.8%)归类为低风险,135 例 pts(36.2%)为高风险。中位随访时间为 41.6 个月。与 EPclin 低风险患者相比,EPclin 高风险患者的疾病复发或死亡风险高两倍(风险比(HR)为 2.05(95%置信区间 0.85-4.96;p=0.110)。EPclin 高风险患者发生远处转移的风险显著高于 EPclin 低风险患者(HR 5.18;95%置信区间 1.04-25.74;p=0.0443)。实际接受辅助 CTX 的 EPclin 高风险患者的 3 年 DFS 为 96.3%(95%置信区间 92.2-100),而未接受 CTX 的 EPclin 高风险患者的 3 年 DFS 为 91.5%(95%置信区间 82.7-100%)(HR 0.32;95%置信区间 0.10-1.05;p=0.061)。
这些前瞻性结局结果表明,EP 在临床常规中是一种有效的临床分子检测方法,可预测 DFS,并指导 ER 阳性、HER2 阴性、淋巴结 0-3 阳性的早期乳腺癌患者使用辅助 CTX 的决策。辅助 CTX 似乎对 EPclin 高风险患者有益。