Icahn School of Medicine at Mount Sinai, Departments of Family Medicine and Community Health and of Population Health Science and Policy, One Gustave L Levy Place, Box 1077, New York, NY 10029, USA
Lund University, Centre for Primary Health Care Research, Clinical Research Centre, Skåne University Hospital, Malmö, Sweden.
BMJ. 2019 May 1;365:l1346. doi: 10.1136/bmj.l1346.
To investigate the relation between preterm birth (gestational age <37 weeks) and risk of CKD from childhood into mid-adulthood.
National cohort study.
Sweden.
4 186 615 singleton live births in Sweden during 1973-2014.
Gestational age at birth, identified from nationwide birth records in the Swedish birth registry.
CKD, identified from nationwide inpatient and outpatient diagnoses through 2015 (maximum age 43 years). Cox regression was used to examine gestational age at birth and risk of CKD while adjusting for potential confounders, and co-sibling analyses assessed the influence of unmeasured shared familial (genetic or environmental) factors.
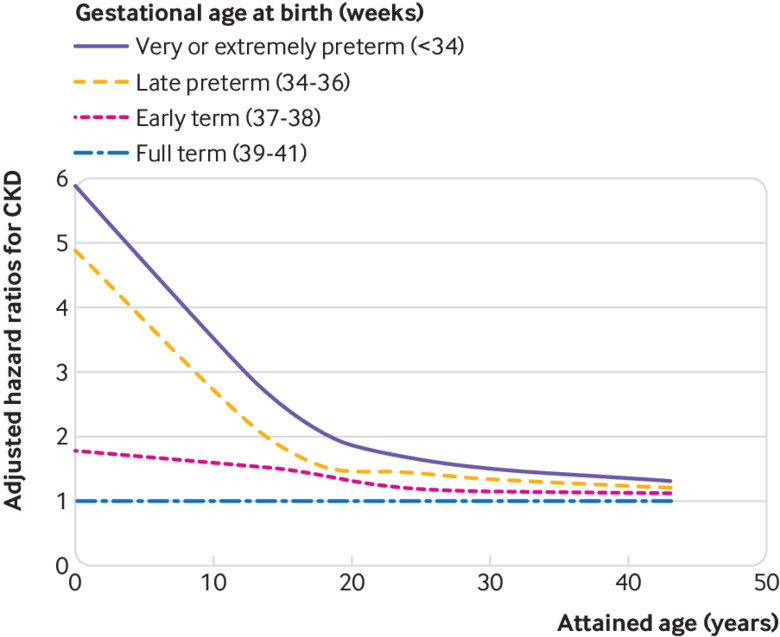
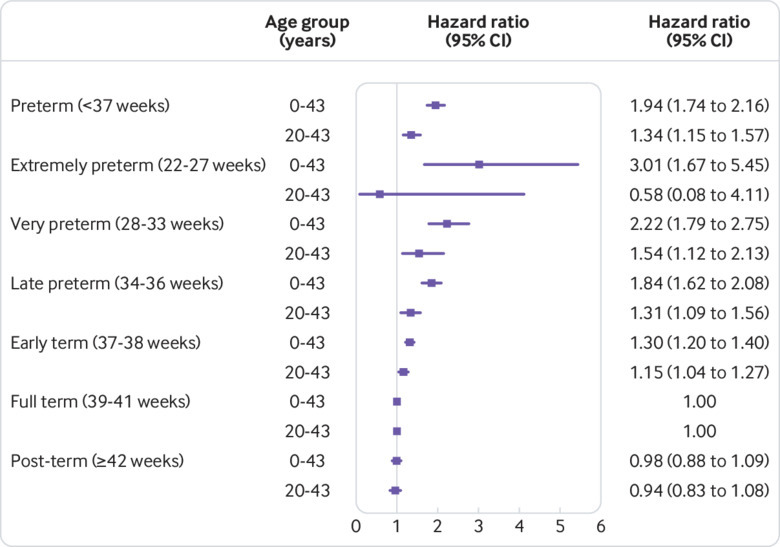
4305 (0.1%) participants had a diagnosis of CKD during 87.0 million person years of follow-up. Preterm birth and extremely preterm birth (<28 weeks) were associated with nearly twofold and threefold risks of CKD, respectively, from birth into mid-adulthood (adjusted hazard ratio 1.94, 95% confidence interval 1.74 to 2.16; P<0.001; 3.01, 1.67 to 5.45; P<0.001). An increased risk was observed even among those born at early term (37-38 weeks) (1.30, 1.20 to 1.40; P<0.001). The association between preterm birth and CKD was strongest at ages 0-9 years (5.09, 4.11 to 6.31; P<0.001), then weakened but remained increased at ages 10-19 years (1.97, 1.57 to 2.49; P<0.001) and 20-43 years (1.34, 1.15 to 1.57; P<0.001). These associations affected both males and females and did not seem to be related to shared genetic or environmental factors in families.
Preterm and early term birth are strong risk factors for the development of CKD from childhood into mid-adulthood. People born prematurely need long term follow-up for monitoring and preventive actions to preserve renal function across the life course.
探讨从儿童期到成年中期早产(胎龄<37 周)与慢性肾脏病(CKD)风险的关系。
全国队列研究。
瑞典。
1973 年至 2014 年期间,瑞典全国范围内出生的 4186615 名单胎活产儿。
胎龄,通过全国性出生记录在瑞典出生登记处确定。
CKD 通过 2015 年之前的全国性住院和门诊诊断确定(最大年龄 43 岁)。使用 Cox 回归来研究胎龄与 CKD 风险之间的关系,同时调整潜在的混杂因素,同胞对照分析评估未测量的共享家族(遗传或环境)因素的影响。
在 8700 万个人年的随访中,4305 名(0.1%)参与者被诊断为 CKD。早产和极早产(<28 周)与儿童期到成年中期 CKD 的风险分别接近两倍和三倍相关(校正后的危险比 1.94,95%置信区间 1.74 至 2.16;P<0.001;3.01,1.67 至 5.45;P<0.001)。即使是在足月产(37-38 周)的人群中也观察到了较高的风险(1.30,1.20 至 1.40;P<0.001)。早产与 CKD 之间的关联在 0-9 岁年龄组最强(5.09,4.11 至 6.31;P<0.001),然后减弱,但在 10-19 岁(1.97,1.57 至 2.49;P<0.001)和 20-43 岁(1.34,1.15 至 1.57;P<0.001)年龄组仍持续增加。这些关联影响了男性和女性,并且似乎与家庭中共享的遗传或环境因素无关。
早产和足月产是儿童期到成年中期 CKD 发展的强烈危险因素。早产儿需要长期随访,以监测和采取预防措施,以保护整个生命周期的肾功能。