Division of Anaesthesia, Addenbrooke's Hospital, University of Cambridge, Cambridge, UK.
Department of Surgery, Rady Faculty of Health Sciences, University of Manitoba, Winnipeg, MB, R3A 1R9, Canada.
Acta Neurochir (Wien). 2019 Jul;161(7):1275-1284. doi: 10.1007/s00701-019-03915-3. Epub 2019 May 3.
Compensatory-reserve-weighted intracranial pressure (wICP) has recently been suggested as a supplementary measure of intracranial pressure (ICP) in adult traumatic brain injury (TBI), with a single-center study suggesting an association with mortality at 6 months. No multi-center studies exist to validate this relationship. The goal was to compare wICP to ICP for association with outcome in a multi-center TBI cohort.
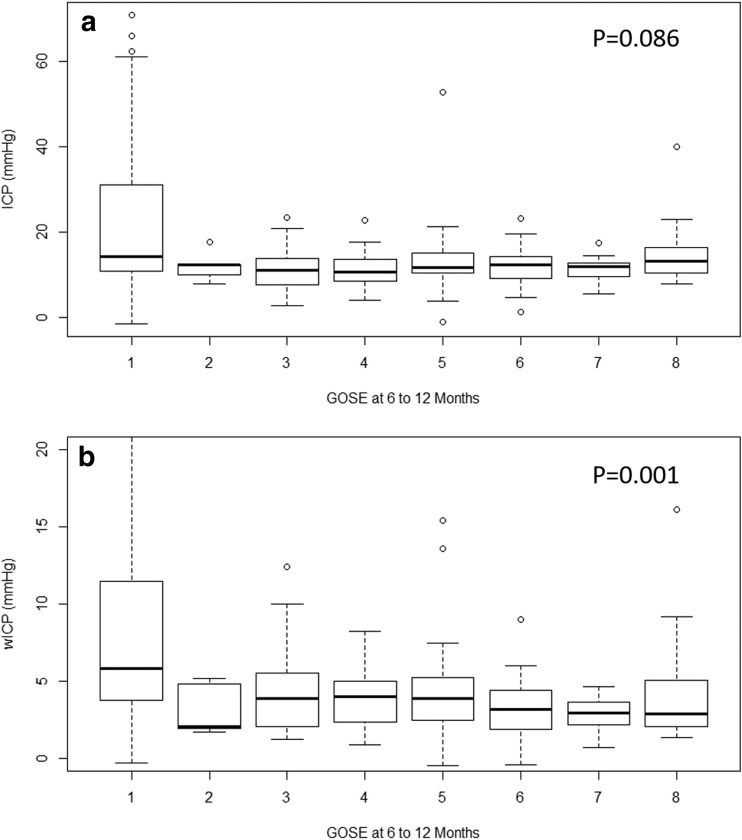
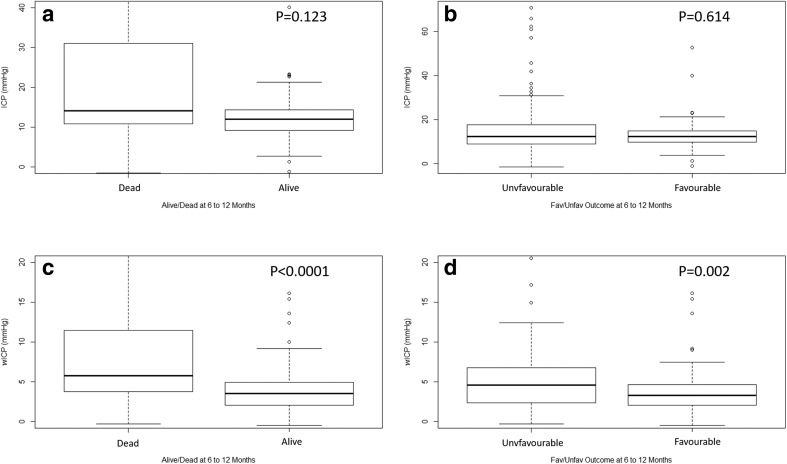
Using the Collaborative European Neuro Trauma Effectiveness Research in TBI (CENTER-TBI) high-resolution intensive care unit (ICU) cohort, we derived ICP and wICP (calculated as wICP = (1 - RAP) × ICP; where RAP is the compensatory reserve index derived from the moving correlation between pulse amplitude of ICP and ICP). Various univariate logistic regression models were created comparing ICP and wICP to dichotomized outcome at 6 to 12 months, based on Glasgow Outcome Score-Extended (GOSE) (alive/dead-GOSE ≥ 2/GOSE = 1; favorable/unfavorable-GOSE 5 to 8/GOSE 1 to 4, respectively). Models were compared using area under the receiver operating curves (AUC) and p values.
wICP displayed higher AUC compared to ICP on univariate regression for alive/dead outcome compared to mean ICP (AUC 0.712, 95% CI 0.615-0.810, p = 0.0002, and AUC 0.642, 95% CI 0.538-746, p < 0.0001, respectively; no significant difference on Delong's test), and for favorable/unfavorable outcome (AUC 0.627, 95% CI 0.548-0.705, p = 0.015, and AUC 0.495, 95% CI 0.413-0.577, p = 0.059; significantly different using Delong's test p = 0.002), with lower wICP values associated with improved outcomes (p < 0.05 for both). These relationships on univariate analysis held true even when comparing the wICP models with those containing both ICP and RAP integrated area under the curve over time (p < 0.05 for all via Delong's test).
Compensatory-reserve-weighted ICP displays superior outcome association for both alive/dead and favorable/unfavorable dichotomized outcomes in adult TBI, through univariate analysis. Lower wICP is associated with better global outcomes. The results of this study provide multi-center validation of those seen in a previous single-center study.
最近有人提出,补偿储备加权颅内压(wICP)可作为成人创伤性脑损伤(TBI)颅内压(ICP)的补充测量指标,一项单中心研究表明,它与 6 个月时的死亡率有关。目前尚无多中心研究来验证这种相关性。本研究的目的是比较 wICP 和 ICP 与多中心 TBI 队列的结局的相关性。
利用协作欧洲神经创伤效应研究在 TBI(CENTER-TBI)高分辨率重症监护病房(ICU)队列,我们得出了 ICP 和 wICP(计算方法为 wICP=(1-RAP)×ICP;其中 RAP 是从 ICP 和 ICP 的脉搏幅度移动相关性中得出的补偿储备指数)。基于格拉斯哥结局量表扩展版(GOSE),我们使用各种单变量逻辑回归模型将 ICP 和 wICP 与 6 至 12 个月的二分法结局进行了比较(存活/死亡-GOSE≥2/GOSE=1;良好/不良-GOSE 5 至 8/GOSE 1 至 4)。使用接受者操作特征曲线下的面积(AUC)和 p 值来比较模型。
与平均 ICP 相比,wICP 在单变量回归中用于存活/死亡结局的 AUC 高于 ICP(AUC 0.712,95%CI 0.615-0.810,p=0.0002,AUC 0.642,95%CI 0.538-746,p<0.0001,分别;Delong 检验无显著差异),对于良好/不良结局(AUC 0.627,95%CI 0.548-0.705,p=0.015,AUC 0.495,95%CI 0.413-0.577,p=0.059;Delong 检验 p=0.002 有显著差异),wICP 值越低,结局越好(两者均为 p<0.05)。即使将包含 ICP 和 RAP 整合曲线下面积的 wICP 模型与那些模型进行比较,这些单变量分析中的关系仍然成立(通过 Delong 检验,所有结果均为 p<0.05)。
在成人 TBI 中,通过单变量分析,补偿储备加权 ICP 对存活/死亡和良好/不良二分法结局的关联具有更好的结果。较低的 wICP 与更好的整体结果相关。本研究的结果提供了对先前单中心研究的多中心验证。