Department of Sexual Health and HIV, Birmingham University Hospitals NHS Foundation Trust, Birmingham, UK.
Nottingham Clinical Trials Unit, University of Nottingham, Queen's Medical Centre, Nottingham, UK.
Lancet. 2019 Jun 22;393(10190):2511-2520. doi: 10.1016/S0140-6736(18)32817-4. Epub 2019 May 2.
Gonorrhoea is a common sexually transmitted infection for which ceftriaxone is the current first-line treatment, but antimicrobial resistance is emerging. The objective of this study was to assess the effectiveness of gentamicin as an alternative to ceftriaxone (both combined with azithromycin) for treatment of gonorrhoea.
G-ToG was a multicentre, parallel-group, pragmatic, randomised, non-inferiority trial comparing treatment with gentamicin to treatment with ceftriaxone for patients with gonorrhoea. The patients, treating physician, and assessing physician were masked to treatment but the treating nurse was not. The trial took place at 14 sexual health clinics in England. Adults aged 16-70 years were eligible for participation if they had a diagnosis of uncomplicated genital, pharyngeal, or rectal gonorrhoea. Participants were randomly assigned to receive a single intramuscular dose of either gentamicin 240 mg (gentamicin group) or ceftriaxone 500 mg (ceftriaxone group). All participants also received a single 1 g dose of oral azithromycin. Randomisation (1:1) was stratified by clinic and performed using a secure web-based system. The primary outcome was clearance of Neisseria gonorrhoeae at all initially infected sites, defined as a negative nucleic acid amplification test 2 weeks post treatment. Primary outcome analyses included only participants who had follow-up data, irrespective of the baseline visit N gonorrhoeae test result. The margin used to establish non-inferiority was a lower confidence limit of 5% for the risk difference. This trial is registered with ISRCTN, number ISRCTN51783227.
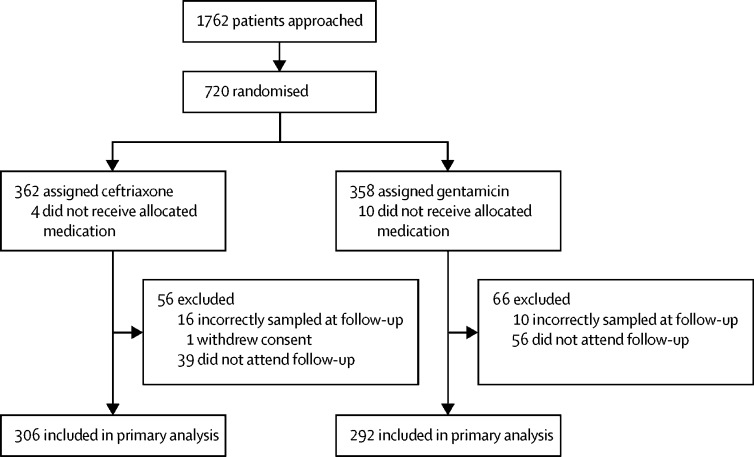
Of 1762 patients assessed, we enrolled 720 participants between Oct 7, 2014, and Nov 14, 2016, and randomly assigned 358 to gentamicin and 362 to ceftriaxone. Primary outcome data were available for 306 (85%) of 362 participants allocated to ceftriaxone and 292 (82%) of 358 participants allocated to gentamicin. At 2 weeks after treatment, infection had cleared for 299 (98%) of 306 participants in the ceftriaxone group compared with 267 (91%) of 292 participants in the gentamicin group (adjusted risk difference -6·4%, 95% CI -10·4% to -2·4%). Of the 328 participants who had a genital infection, 151 (98%) of 154 in the ceftriaxone group and 163 (94%) of 174 in the gentamicin group had clearance at follow-up (adjusted risk difference -4·4%, -8·7 to 0). For participants with a pharyngeal infection, a greater proportion receiving ceftriaxone had clearance at follow-up (108 [96%] in the ceftriaxone group compared with 82 [80%] in the gentamicin group; adjusted risk difference -15·3%, -24·0 to -6·5). Similarly, a greater proportion of participants with rectal infection in the ceftriaxone group had clearance (134 [98%] in the ceftriaxone group compared with 107 [90%] in the gentamicin group; adjusted risk difference -7·8%, -13·6 to -2·0). Thus, we did not find that a single dose of gentamicin 240 mg was non-inferior to a single dose of ceftriaxone 500 mg for the treatment of gonorrhoea, when both drugs were combined with a 1 g dose of oral azithromycin. The side-effect profiles were similar between groups, although severity of pain at the injection site was higher for gentamicin (mean visual analogue pain score 36 of 100 in the gentamicin group vs 21 of 100 in the ceftriaxone group).
Gentamicin is not appropriate as first-line treatment for gonorrhoea but remains potentially useful for patients with isolated genital infection, or for patients who are allergic or intolerant to ceftriaxone, or harbour a ceftriaxone-resistant isolate. Further research is required to identify and test new alternatives to ceftriaxone for the treatment of gonorrhoea.
UK National Institute for Health Research.
淋病是一种常见的性传播感染,目前头孢曲松是一线治疗药物,但抗菌药物耐药性正在出现。本研究的目的是评估庆大霉素替代头孢曲松(两者均与阿奇霉素联合使用)治疗淋病的疗效。
G-ToG 是一项多中心、平行组、实用、随机、非劣效性试验,比较了庆大霉素和头孢曲松治疗淋病患者的效果。患者、治疗医生和评估医生对治疗情况均不知情,但治疗护士知情。试验在英国 14 家性健康诊所进行。年龄在 16-70 岁之间、诊断为单纯性生殖器、咽或直肠淋病的成年人有资格参加。参与者随机分配接受单次肌内注射庆大霉素 240mg(庆大霉素组)或头孢曲松 500mg(头孢曲松组)。所有参与者还接受单次 1g 剂量的口服阿奇霉素。随机分组(1:1)按诊所分层,并使用安全的基于网络的系统进行。主要结局是所有最初感染部位的淋病奈瑟菌清除,定义为治疗后 2 周时核酸扩增试验阴性。主要结局分析仅包括有随访数据的参与者,无论基线访视 N 淋病奈瑟菌检测结果如何。用于建立非劣效性的界限是风险差异的置信下限为 5%。本试验在 ISRCTN 注册,编号 ISRCTN51783227。
在评估的 1762 名患者中,我们于 2014 年 10 月 7 日至 2016 年 11 月 14 日期间纳入了 720 名参与者,并随机分配 358 名参与者接受庆大霉素治疗,362 名参与者接受头孢曲松治疗。我们获得了 306 名(85%)分配给头孢曲松的 362 名参与者和 292 名(82%)分配给庆大霉素的 358 名参与者的主要结局数据。治疗后 2 周时,头孢曲松组 306 名参与者中有 299 名(98%)感染清除,庆大霉素组 292 名参与者中有 267 名(91%)感染清除(调整后的风险差异-6.4%,95%CI-10.4%至-2.4%)。在 328 名患有生殖器感染的参与者中,头孢曲松组 151 名(98%)和庆大霉素组 163 名(94%)在随访时清除感染(调整后的风险差异-4.4%,-8.7 至 0)。对于患有咽感染的参与者,接受头孢曲松治疗的参与者中有更高比例在随访时清除感染(头孢曲松组 108 名[96%]与庆大霉素组 82 名[80%])(调整后的风险差异-15.3%,-24.0 至-6.5%)。同样,头孢曲松组中患有直肠感染的参与者中有更高比例清除感染(头孢曲松组 134 名[98%]与庆大霉素组 107 名[90%])(调整后的风险差异-7.8%,-13.6 至-2.0%)。因此,我们发现,当头孢曲松和阿奇霉素联合使用时,单次庆大霉素 240mg 治疗淋病并不优于单次头孢曲松 500mg,不能作为淋病的一线治疗药物。两组的副作用谱相似,但庆大霉素注射部位疼痛的严重程度更高(庆大霉素组平均视觉模拟疼痛评分 36 分,头孢曲松组为 21 分)。
庆大霉素不适合作为淋病的一线治疗药物,但对单纯性生殖器感染、对头孢曲松过敏或不耐受、或感染头孢曲松耐药株的患者仍有潜在用途。需要进一步研究以确定和测试治疗淋病的头孢曲松新替代药物。
英国国家卫生研究院。