Kim Young Zoon, Kim Chae Yong, Lim Jaejoon, Sung Kyoung Su, Lee Jihae, Oh Hyuk Jin, Kang Seok Gu, Kang Shin Hyuk, Kong Doo Sik, Kim Sung Hwan, Kim Se Hyuk, Kim Se Hoon, Kim Yu Jung, Kim Eui Hyun, Kim In Ah, Kim Ho Sung, Roh Tae Hoon, Park Jae Sung, Park Hyun Jin, Song Sang Woo, Yang Seung Ho, Yoon Wan Soo, Yoon Hong In, Lee Soon Tae, Lee Sea Won, Lee Youn Soo, Wee Chan Woo, Chang Jong Hee, Jung Tae Young, Jung Hye Lim, Cho Jae Ho, Choi Seung Hong, Choi Hyoung Soo, Hong Je Beom, Lim Do Hoon, Chung Dong Sup
Division of Neurooncology and Department of Neurosurgery, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Korea.
Department of Neurosurgery, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea.
Brain Tumor Res Treat. 2019 Apr;7(1):1-9. doi: 10.14791/btrt.2019.7.e25.
There has been no practical guidelines for the management of patients with central nervous system (CNS) tumors in Korea for many years. Thus, the Korean Society for Neuro-Oncology (KSNO), a multidisciplinary academic society, started to prepare guidelines for CNS tumors from February 2018.
The Working Group was composed of 35 multidisciplinary medical experts in Korea. References were identified through searches of PubMed, MEDLINE, EMBASE, and Cochrane CENTRAL using specific and sensitive keywords as well as combinations of keywords.
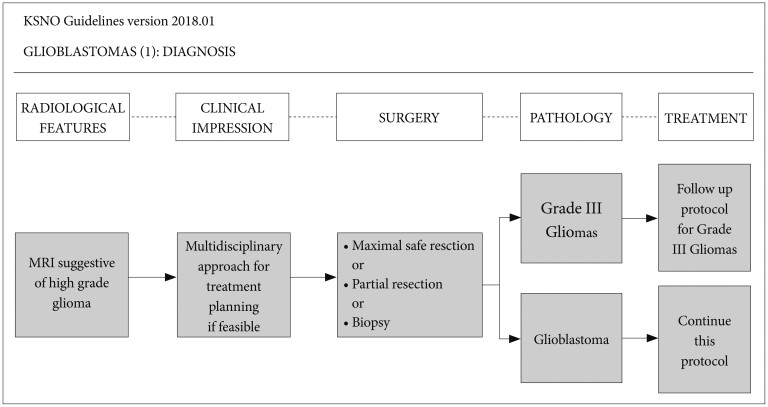
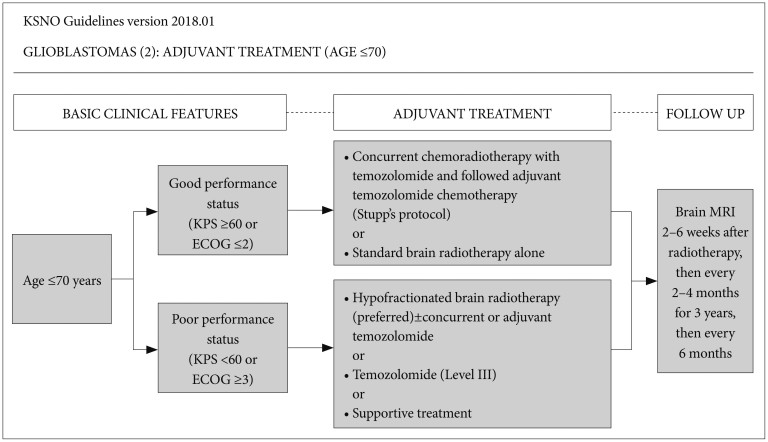
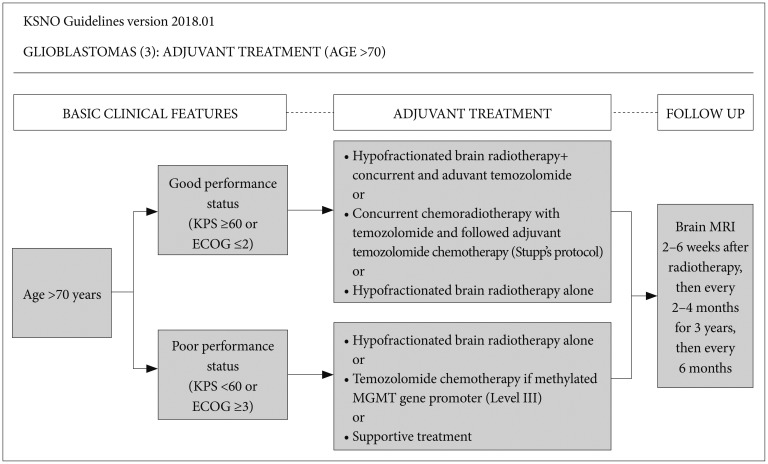
First, the maximal safe resection if feasible is recommended. After the diagnosis of a glioblastoma with neurosurgical intervention, patients aged ≤70 years with good performance should be treated by concurrent chemoradiotherapy with temozolomide followed by adjuvant temozolomide chemotherapy (Stupp's protocol) or standard brain radiotherapy alone. However, those with poor performance should be treated by hypofractionated brain radiotherapy (preferred)±concurrent or adjuvant temozolomide, temozolomide alone (Level III), or supportive treatment. Alternatively, patients aged >70 years with good performance should be treated by hypofractionated brain radiotherapy+concurrent and adjuvant temozolomide or Stupp's protocol or hypofractionated brain radiotherapy alone, while those with poor performance should be treated by hypofractionated brain radiotherapy alone or temozolomide chemotherapy if the patient has methylated MGMT gene promoter (Level III), or supportive treatment.
The KSNO's guideline recommends that glioblastomas should be treated by maximal safe resection, if feasible, followed by radiotherapy and/or chemotherapy according to the individual comprehensive condition of the patient.
多年来,韩国一直没有关于中枢神经系统(CNS)肿瘤患者管理的实用指南。因此,多学科的学术团体韩国神经肿瘤学会(KSNO)于2018年2月开始制定CNS肿瘤指南。
工作组由韩国35名多学科医学专家组成。通过使用特定且敏感的关键词以及关键词组合在PubMed、MEDLINE、EMBASE和Cochrane CENTRAL中进行检索来确定参考文献。
首先,建议在可行的情况下进行最大安全切除。在经神经外科干预诊断为胶质母细胞瘤后,年龄≤70岁、身体状况良好的患者应接受替莫唑胺同步放化疗,随后进行替莫唑胺辅助化疗(Stupp方案)或单纯标准脑放疗。然而,身体状况较差的患者应接受低分割脑放疗(首选)±同步或辅助替莫唑胺、单纯替莫唑胺治疗(三级)或支持治疗。另外,年龄>70岁、身体状况良好的患者应接受低分割脑放疗+同步和辅助替莫唑胺或Stupp方案或单纯低分割脑放疗,而身体状况较差的患者如果其MGMT基因启动子甲基化,应接受单纯低分割脑放疗或替莫唑胺化疗(三级),或支持治疗。
KSNO指南建议,胶质母细胞瘤如果可行应通过最大安全切除进行治疗,然后根据患者的个体综合情况进行放疗和/或化疗。