Kim Young Zoon, Kim Chae Yong, Wee Chan Woo, Roh Tae Hoon, Hong Je Beom, Oh Hyuk Jin, Kang Seok Gu, Kang Shin Hyuk, Kong Doo Sik, Kim Sung Hwan, Kim Se Hyuk, Kim Se Hoon, Kim Yu Jung, Kim Eui Hyun, Kim In Ah, Kim Ho Sung, Park Jae Sung, Park Hyun Jin, Song Sang Woo, Sung Kyoung Su, Yang Seung Ho, Yoon Wan Soo, Yoon Hong In, Lee Jihae, Lee Soon Tae, Lee Sea Won, Lee Youn Soo, Lim Jaejoon, Chang Jong Hee, Jung Tae Young, Jung Hye Lim, Cho Jae Ho, Choi Seung Hong, Choi Hyoung Soo, Lim Do Hoon, Chung Dong Sup
Division of Neurooncology and Department of Neurosurgery, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Korea.
Department of Neurosurgery, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea.
Brain Tumor Res Treat. 2019 Oct;7(2):74-84. doi: 10.14791/btrt.2019.7.e43.
There was no practical guideline for the management of patients with central nervous system tumor in Korea for many years. Thus, the Korean Society for Neuro-Oncology (KSNO), a multidisciplinary academic society, has developed the guideline for glioblastoma. Subsequently, the KSNO guideline for World Health Organization (WHO) grade II cerebral glioma in adults is established.
The Working Group was composed of 35 multidisciplinary medical experts in Korea. References were identified by searching PubMed, MEDLINE, EMBASE, and Cochrane CENTRAL databases using specific and sensitive keywords as well as combinations of keywords regarding diffuse astrocytoma and oligodendroglioma of brain in adults.
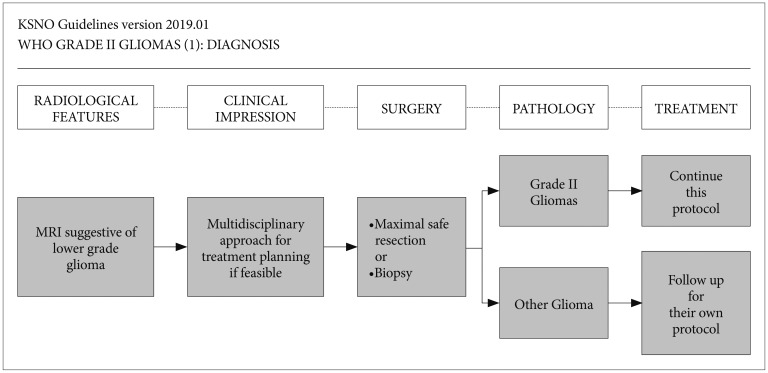
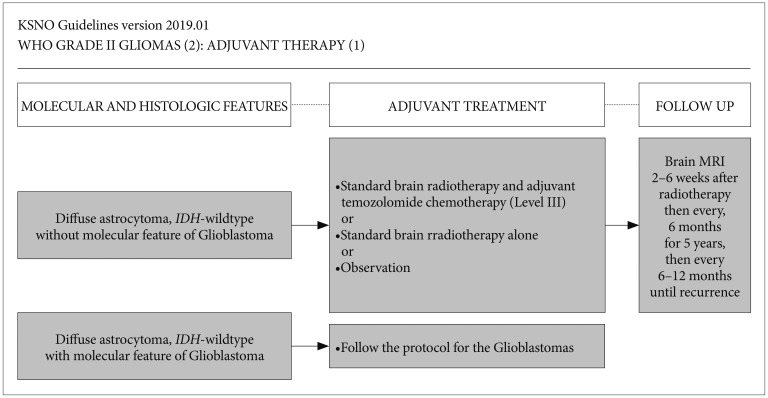
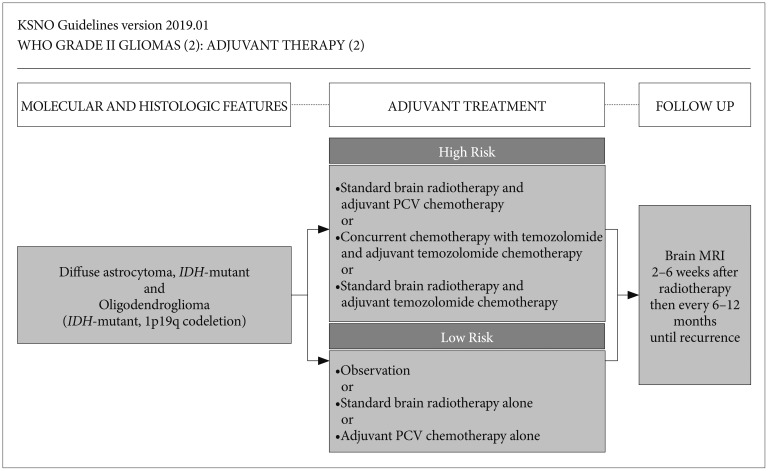
Whenever radiological feature suggests lower grade glioma, the maximal safe resection if feasible is recommended globally. After molecular and histological examinations, patients with diffuse astrocytoma, isocitrate dehydrogenase ()-wildtype without molecular feature of glioblastoma should be primarily treated by standard brain radiotherapy and adjuvant temozolomide chemotherapy (Level III) while those with molecular feature of glioblastoma should be treated following the protocol for glioblastomas. In terms of patients with diffuse astrocytoma, -mutant and oligodendroglioma (-mutant and 1p19q codeletion), standard brain radiotherapy and adjuvant PCV (procarbazine+lomustine+vincristine) combination chemotherapy should be considered primarily for the high-risk group while observation with regular follow up should be considered for the low-risk group.
The KSNO's guideline recommends that WHO grade II gliomas should be treated by maximal safe resection, if feasible, followed by radiotherapy and/or chemotherapy according to molecular and histological features of tumors and clinical characteristics of patients.
多年来韩国一直没有针对中枢神经系统肿瘤患者管理的实用指南。因此,多学科的学术团体韩国神经肿瘤学会(KSNO)制定了胶质母细胞瘤指南。随后,KSNO又制定了成人世界卫生组织(WHO)二级脑胶质瘤指南。
工作组由韩国35名多学科医学专家组成。通过使用特定且敏感的关键词以及关于成人脑弥漫性星形细胞瘤和少突胶质细胞瘤的关键词组合,在PubMed、MEDLINE、EMBASE和Cochrane CENTRAL数据库中进行检索以确定参考文献。
无论何时放射学特征提示为低级别胶质瘤,全球均推荐在可行的情况下进行最大安全切除。经过分子和组织学检查后,对于弥漫性星形细胞瘤、异柠檬酸脱氢酶()野生型且无胶质母细胞瘤分子特征的患者,应首先采用标准脑放疗和辅助替莫唑胺化疗(三级证据),而具有胶质母细胞瘤分子特征的患者应按照胶质母细胞瘤治疗方案进行治疗。对于弥漫性星形细胞瘤、-突变型和少突胶质细胞瘤(-突变型和1p19q共缺失)患者,高危组应主要考虑标准脑放疗和辅助PCV(丙卡巴肼+洛莫司汀+长春新碱)联合化疗,低危组应考虑定期随访观察。
KSNO指南建议,对于WHO二级胶质瘤,如果可行,应进行最大安全切除,然后根据肿瘤的分子和组织学特征以及患者的临床特征进行放疗和/或化疗。