Yoon Hong In, Wee Chan Woo, Kim Young Zoon, Seo Youngbeom, Im Jung Ho, Dho Yun Sik, Kim Kyung Hwan, Hong Je Beom, Park Jae Sung, Choi Seo Hee, Kim Min Sung, Moon Jangsup, Hwang Kihwan, Park Ji Eun, Cho Jin Mo, Yoon Wan Soo, Kim Se Hoon, Kim Young Il, Kim Ho Sung, Sung Kyoung Su, Song Jin Ho, Lee Min Ho, Han Myung Hoon, Lee Se Hoon, Chang Jong Hee, Lim Do Hoon, Park Chul Kee, Lee Youn Soo, Gwak Ho Shin
Department of Radiation Oncology, Yonsei Cancer Center, Yonsei University College of Medicine, Seoul, Korea.
Department of Radiation Oncology, SMG-SNU Boramae Medical Center, Seoul, Korea.
Brain Tumor Res Treat. 2021 Apr;9(1):1-8. doi: 10.14791/btrt.2021.9.e8.
There have been no guidelines for the management of adult patients with diffuse midline glioma (DMG), H3K27M-mutant in Korea since the 2016 revised WHO classification newly defined this disease entity. Thus, the Korean Society for Neuro-Oncology (KSNO), a multidisciplinary academic society, had begun preparing guidelines for DMG since 2019.
The Working Group was composed of 27 multidisciplinary medical experts in Korea. References were identified through searches of PubMed, MEDLINE, EMBASE, and Cochrane CENTRAL using specific and sensitive keywords as well as combinations of keywords. As 'diffuse midline glioma' was recently defined, and there was no international guideline, trials and guidelines of 'diffuse intrinsic pontine glioma' or 'brain stem glioma' were thoroughly reviewed first.
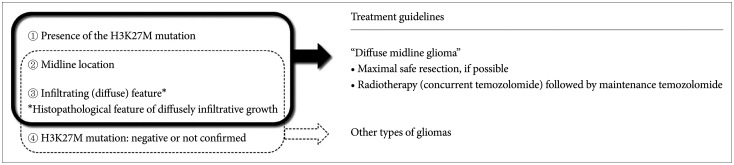
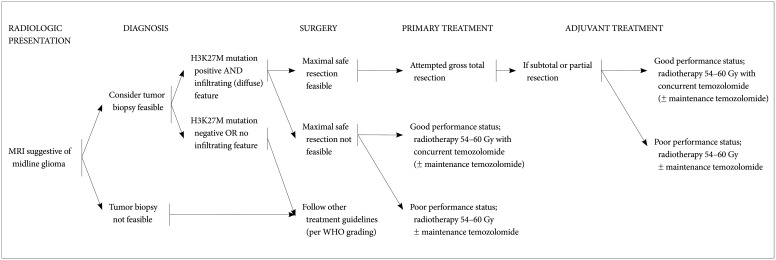
The core contents are as follows. The DMG can be diagnosed when all of the following three criteria are satisfied: the presence of the H3K27M mutation, midline location, and infiltrating feature. Without identification of H3K27M mutation by diagnostic biopsy, DMG cannot be diagnosed. For the primary treatment, maximal safe resection should be considered for tumors when feasible. Radiotherapy is the primary option for tumors in case the total resection is not possible. A total dose of 54 Gy to 60 Gy with conventional fractionation prescribed at 1-2 cm plus gross tumor volume is recommended. Although no chemotherapy has proven to be effective in DMG, concurrent chemoradiotherapy (± maintenance chemotherapy) with temozolomide following WHO grade IV glioblastoma's protocol is recommended.
The detection of H3K27M mutation is the most important diagnostic criteria for DMG. Combination of surgery (if amenable to surgery), radiotherapy, and chemotherapy based on comprehensive multidisciplinary discussion can be considered as the treatment options for DMG.
自2016年修订的世界卫生组织分类新定义弥漫性中线胶质瘤(DMG)、H3K27M突变型成人患者以来,韩国尚无针对此类患者的管理指南。因此,多学科学术团体韩国神经肿瘤学会(KSNO)自2019年起开始制定DMG指南。
工作组由韩国27位多学科医学专家组成。通过使用特定且敏感的关键词以及关键词组合在PubMed、MEDLINE、EMBASE和Cochrane CENTRAL中进行检索来确定参考文献。由于“弥漫性中线胶质瘤”是最近定义的,且尚无国际指南,因此首先对“弥漫性脑桥内胶质瘤”或“脑干胶质瘤”的试验和指南进行了全面审查。
核心内容如下。当满足以下所有三个标准时可诊断为DMG:存在H3K27M突变、中线位置和浸润特征。未经诊断性活检鉴定出H3K27M突变,则不能诊断为DMG。对于初始治疗,可行时应考虑对肿瘤进行最大安全切除。如果无法进行全切除,放疗是肿瘤的主要选择。建议采用常规分割方式,总剂量为54 Gy至60 Gy,在大体肿瘤体积外加1 - 2 cm处方剂量。尽管尚无化疗被证明对DMG有效,但建议按照世界卫生组织IV级胶质母细胞瘤的方案,采用替莫唑胺同步放化疗(±维持化疗)。
H3K27M突变的检测是DMG最重要的诊断标准。基于全面多学科讨论的手术(如果适合手术)、放疗和化疗联合可被视为DMG的治疗选择。