Department of Clinical Neurosciences, University of Cambridge, Cambridge, United Kingdom.
Nuffield Department of Clinical Neurosciences and.
JCI Insight. 2019 May 7;5(12):125377. doi: 10.1172/jci.insight.125377.
The lymphocyte-depleting antibody alemtuzumab is a highly effective treatment of relapsing-remitting multiple sclerosis (RRMS); however 50% of patients develop novel autoimmunity post-treatment. Most at risk are individuals who reconstitute their T-cell pool by proliferating residual cells, rather than producing new T-cells in the thymus; raising the possibility that autoimmunity might be prevented by increasing thymopoiesis. Keratinocyte growth factor (palifermin) promotes thymopoiesis in non-human primates.
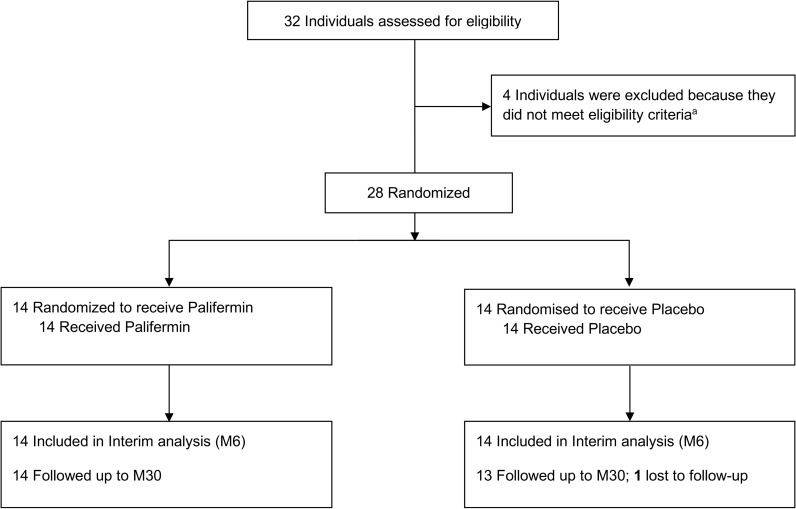
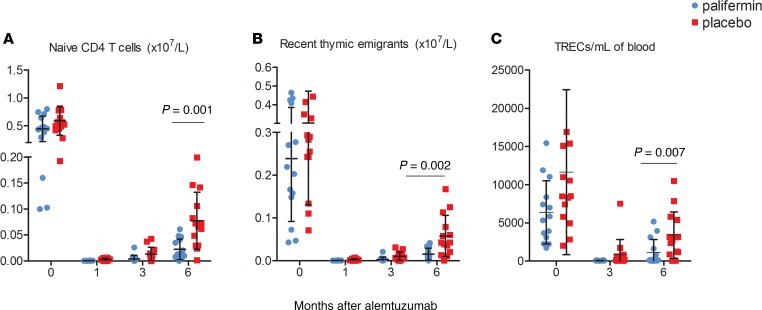
Following a dose-tolerability sub-study, individuals with RRMS (duration ≤10 years; expanded disability status scale ≤5·0; with ≥2 relapses in the previous 2 years) were randomised to placebo or 180mcg/kg/day palifermin, given for 3 days immediately prior to and after each cycle of alemtuzumab, with repeat doses at M1 and M3. The interim primary endpoint was naïve CD4+ T-cell count at M6. Exploratory endpoints included: number of recent thymic-emigrants (RTEs) and signal-joint T-cell receptor excision circles (sjTRECs)/mL of blood. The trial primary endpoint was incidence of autoimmunity at M30.
At M6, individuals receiving palifermin had fewer naïve CD4+T-cells (2.229x107/L vs. 7.733x107/L; p=0.007), RTEs (16% vs. 34%) and sjTRECs/mL (1100 vs. 3396), leading to protocol-defined termination of recruitment. No difference was observed in the rate of autoimmunity between the two groupsConclusion: In contrast to animal studies, palifermin reduced thymopoiesis in our patients. These results offer a note of caution to those using palifermin to promote thymopoiesis in other settings, particularly in the oncology/haematology setting where alemtuzumab is often used as part of the conditioning regime.
ClinicalTrials.gov NCT01712945Funding: MRC and Moulton Charitable Foundation.
淋巴细胞耗竭抗体阿仑单抗是一种治疗复发缓解型多发性硬化症(RRMS)的高度有效药物;然而,50%的患者在治疗后会出现新的自身免疫。风险最高的是那些通过增殖残留细胞而不是在胸腺中产生新 T 细胞来重建 T 细胞池的个体;这就提出了一个可能性,即通过增加胸腺生成来预防自身免疫。角质细胞生长因子(培非格司亭)可促进非人类灵长类动物的胸腺生成。
在一项剂量耐受性亚研究之后,RRMS 个体(病程≤10 年;扩展残疾状态量表≤5.0;在过去 2 年内有≥2 次复发)被随机分配至安慰剂或 180mcg/kg/天培非格司亭组,在每个阿仑单抗周期前 3 天和后 3 天给予培非格司亭,并在 M1 和 M3 时重复给药。中期主要终点是 M6 时的幼稚 CD4+T 细胞计数。探索性终点包括:近期胸腺迁出细胞(RTE)和信号连接 T 细胞受体切除环(sjTRECs)/mL 血液的数量。该试验的主要终点是 M30 时的自身免疫发生率。
在 M6 时,接受培非格司亭的个体幼稚 CD4+T 细胞较少(2.229x107/L 比 7.733x107/L;p=0.007),RTE(16%比 34%)和 sjTRECs/mL(1100 比 3396),导致研究方案终止招募。两组之间的自身免疫发生率没有差异。
与动物研究相反,培非格司亭降低了我们患者的胸腺生成。这些结果为那些在其他情况下使用培非格司亭促进胸腺生成的人敲响了警钟,特别是在肿瘤学/血液学领域,阿仑单抗常作为预处理方案的一部分。
ClinicalTrials.gov NCT01712945 资金来源:MRC 和莫尔顿慈善基金会。