Department of Neurology, Keck School of Medicine, University of Southern California, 1333 San Pablo Street McKibben Hall Room 245A, Los Angeles, CA, 90033, USA.
Department of Molecular Microbiology and Immunology, Keck School of Medicine, University of Southern California, Los Angeles, CA, USA.
J Neuroinflammation. 2020 Jun 15;17(1):189. doi: 10.1186/s12974-020-01847-9.
To characterize long-term repopulation of peripheral immune cells following alemtuzumab-induced lymphopenia in relapsing-remitting MS (RRMS), with a focus on regulatory cell types, and to explore associations with clinical outcome measures.
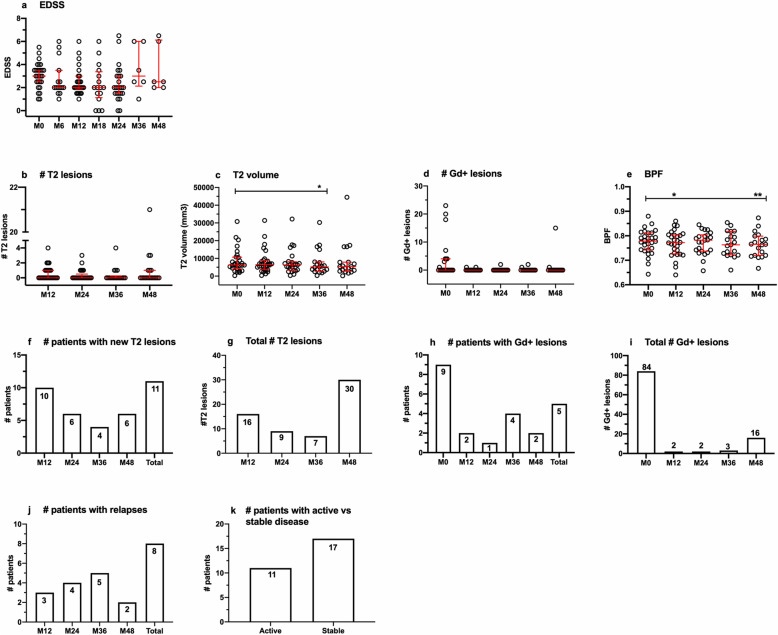
The project was designed as a multicenter add-on longitudinal mechanistic study for RRMS patients enrolled in CARE-MS II, CARE-MS II extension at the University of Southern California and Stanford University, and an investigator-initiated study conducted at the Universities of British Columbia and Chicago. Methods involved collection of blood at baseline, prior to alemtuzumab administration, and at months 5, 11, 17, 23, 36, and 48 post-treatment. T cell, B cell, and natural killer (NK) cell subsets, chemokine receptor expression in T cells, in vitro cytokine secretion patterns, and regulatory T cell (Treg) function were assessed. Clinical outcomes, including expanded disability status score (EDSS), relapses, conventional magnetic resonance imaging (MRI) measures, and incidents of secondary autoimmunity were tracked.
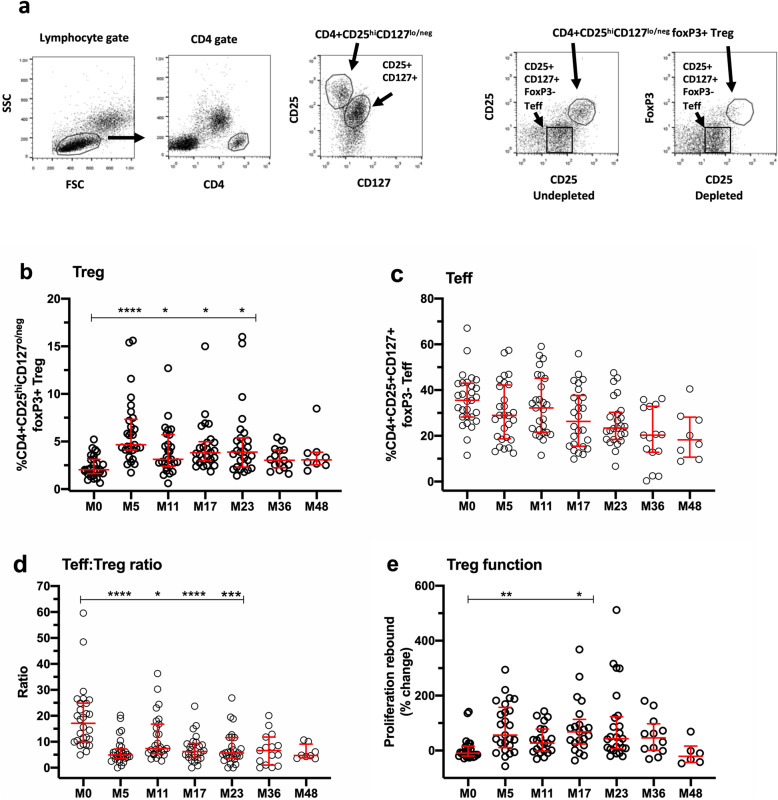
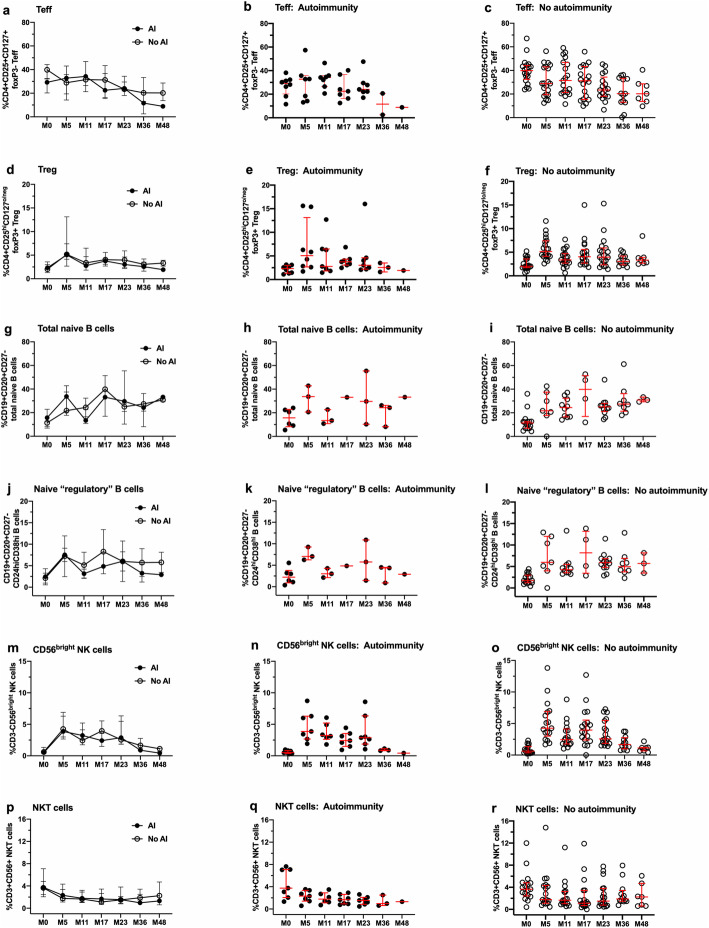
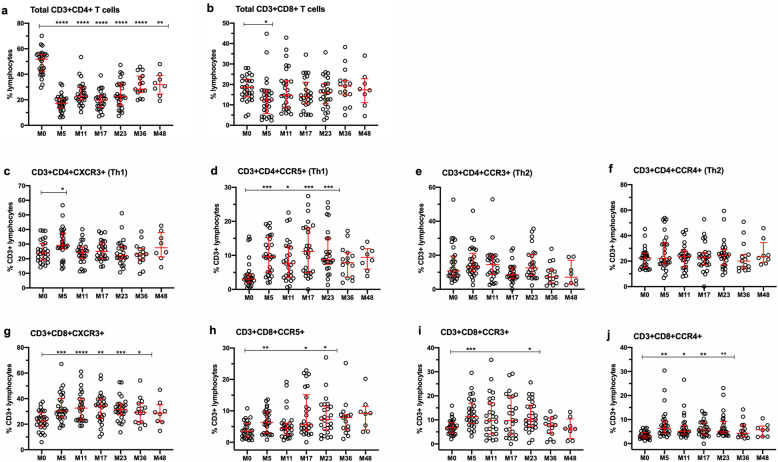
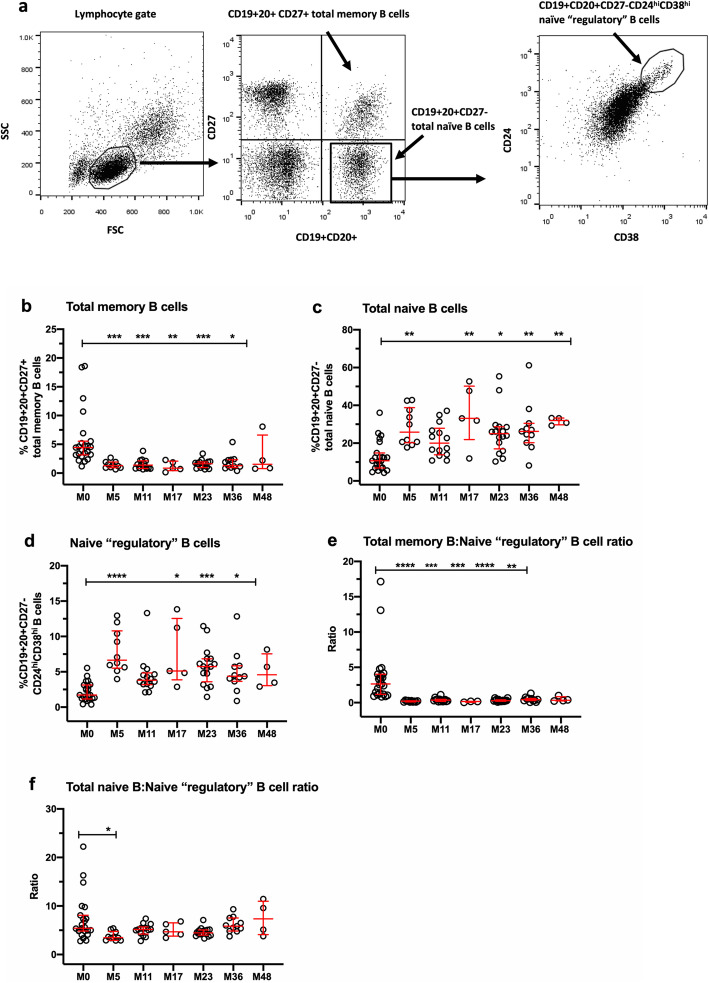
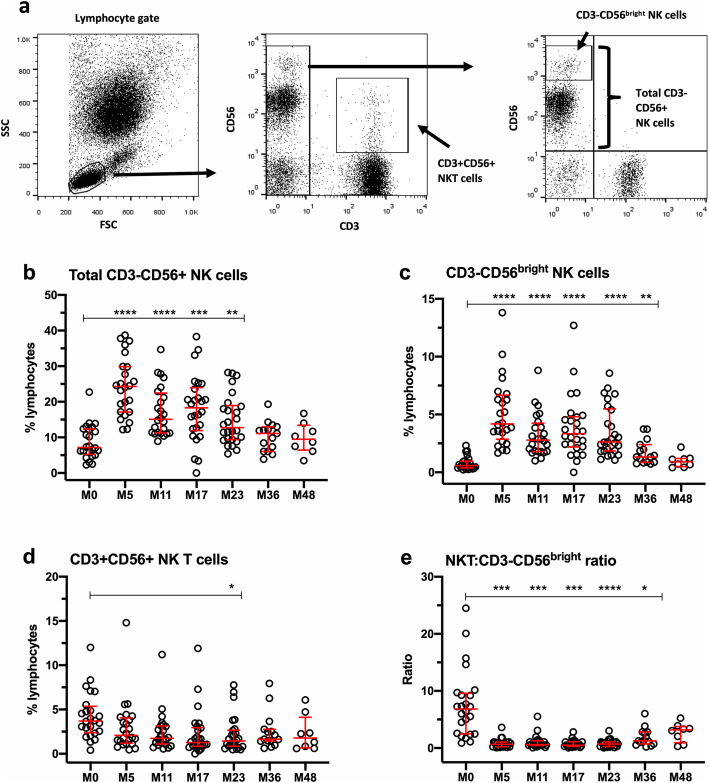
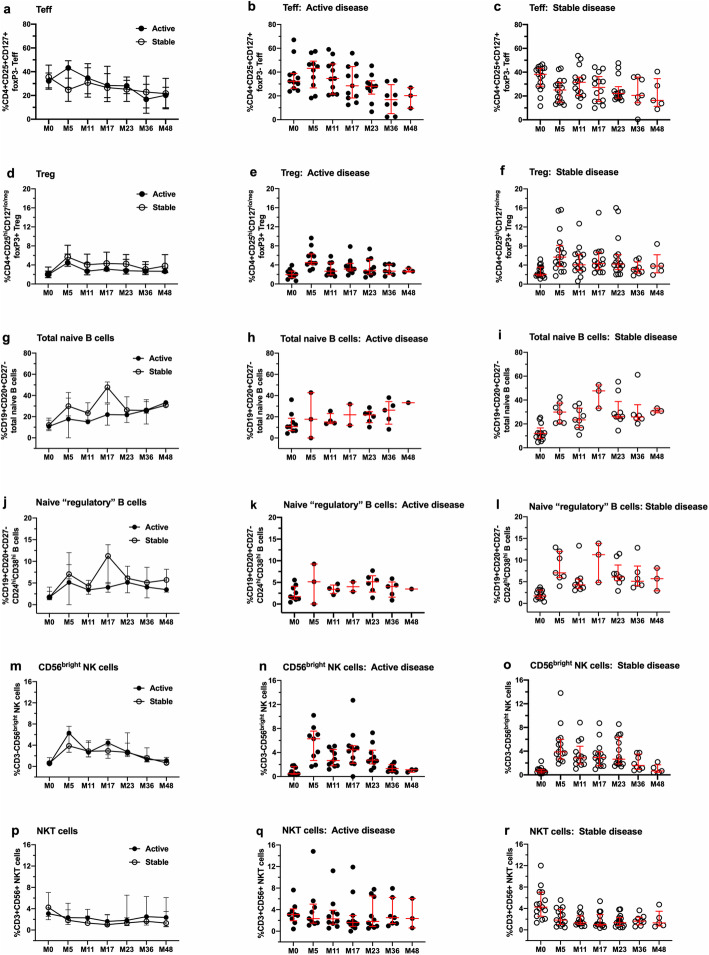
Variable shifts in lymphocyte populations occurred over time in favor of CD4+ T cells, B cells, and NK cells with surface phenotypes characteristic of regulatory subsets, accompanied by reduced ratios of effector to regulatory cell types. Evidence of increased Treg competence was observed after each treatment course. CD4+ and CD8+ T cells that express CXCR3 and CCR5 and CD8+ T cells that express CDR3 and CCR4 were also enriched after treatment, indicating heightened trafficking potential in activated T cells. Patterns of repopulation were not associated with measures of clinical efficacy or secondary autoimmunity, but exploratory analyses using a random generalized estimating equation (GEE) Poisson model provide preliminary evidence of associations between pro-inflammatory cell types and increased risk for gadolinium (Gd+) enhancing lesions, while regulatory subsets were associated with reduced risk. In addition, the risk for T2 lesions correlated with increases in CD3+CD8+CXCR3+ cells.
Lymphocyte repopulation after alemtuzumab treatment favors regulatory subsets in the T cell, B cell, and NK cell compartments. Clinical efficacy may reflect the sum of interactions among them, leading to control of potentially pathogenic effector cell types. Several immune measures were identified as possible biomarkers of lesion activity. Future studies are necessary to more precisely define regulatory and effector subsets and their contributions to clinical efficacy and risk for secondary autoimmunity in alemtuzumab-treated patients, and to reveal new insights into mechanisms of immunopathogenesis in MS.
Parent trials for this study are registered with ClinicalTrials.gov: CARE-MS II: NCT00548405, CARE-MS II extension: NCT00930553 and ISS: NCT01307332.
描述来氟米特诱导的复发缓解型多发性硬化症(RRMS)患者淋巴细胞减少后外周免疫细胞的长期再群体,重点关注调节性细胞类型,并探讨其与临床结果测量的关联。
该项目设计为 RRMS 患者的多中心附加纵向机制研究,包括参与 CARE-MS II、南加州大学和斯坦福大学的 CARE-MS II 扩展以及不列颠哥伦比亚大学和芝加哥大学进行的研究者发起的研究。方法包括在基线、来氟米特治疗前以及治疗后 5、11、17、23、36 和 48 个月收集血液。评估了 T 细胞、B 细胞和自然杀伤 (NK) 细胞亚群、T 细胞中趋化因子受体表达、体外细胞因子分泌模式和调节性 T 细胞 (Treg) 功能。跟踪了临床结果,包括扩展残疾状况评分 (EDSS)、复发、常规磁共振成像 (MRI) 测量以及继发性自身免疫事件。
随着时间的推移,淋巴细胞群发生了变化,有利于具有调节亚群特征的 CD4+T 细胞、B 细胞和 NK 细胞,同时效应细胞与调节细胞类型的比例降低。在每个疗程后观察到 Treg 功能增强的证据。治疗后,表达 CXCR3 和 CCR5 的 CD4+和 CD8+T 细胞以及表达 CDR3 和 CCR4 的 CD8+T 细胞也被富集,表明激活的 T 细胞具有更高的迁移潜力。再群体的模式与临床疗效或继发性自身免疫无关,但使用随机广义估计方程 (GEE) 泊松模型的探索性分析提供了初步证据,表明促炎细胞类型与钆增强病变的风险增加之间存在关联,而调节亚群与风险降低有关。此外,T2 病变的风险与 CD3+CD8+CXCR3+细胞的增加相关。
来氟米特治疗后淋巴细胞的再群体有利于 T 细胞、B 细胞和 NK 细胞中调节亚群。临床疗效可能反映了它们之间相互作用的总和,导致对潜在致病性效应细胞类型的控制。已经确定了几种免疫措施作为病变活动的可能生物标志物。未来的研究有必要更精确地定义调节和效应亚群及其对来氟米特治疗患者的临床疗效和继发性自身免疫风险的贡献,并揭示多发性硬化症免疫发病机制的新见解。
本研究的母体试验在美国临床试验注册处注册:CARE-MS II:NCT00548405、CARE-MS II 扩展:NCT00930553 和 ISS:NCT01307332。