Tesfaye Anteneh A, Wang Hongkun, Hartley Marion L, He Aiwu Ruth, Weiner Louis, Gabelia Nina, Kapanadze Lana, Shezad Muhammad, Brody Jonathan R, Marshall John L, Pishvaian Michael J
Karmanos Cancer Institute, Wayne State University, Detroit, Michigan.
Lombardi Comprehensive Cancer Center, Georgetown University, Washington, District of Columbia.
J Pancreat Cancer. 2019 May 2;5(1):12-21. doi: 10.1089/pancan.2019.0003. eCollection 2019.
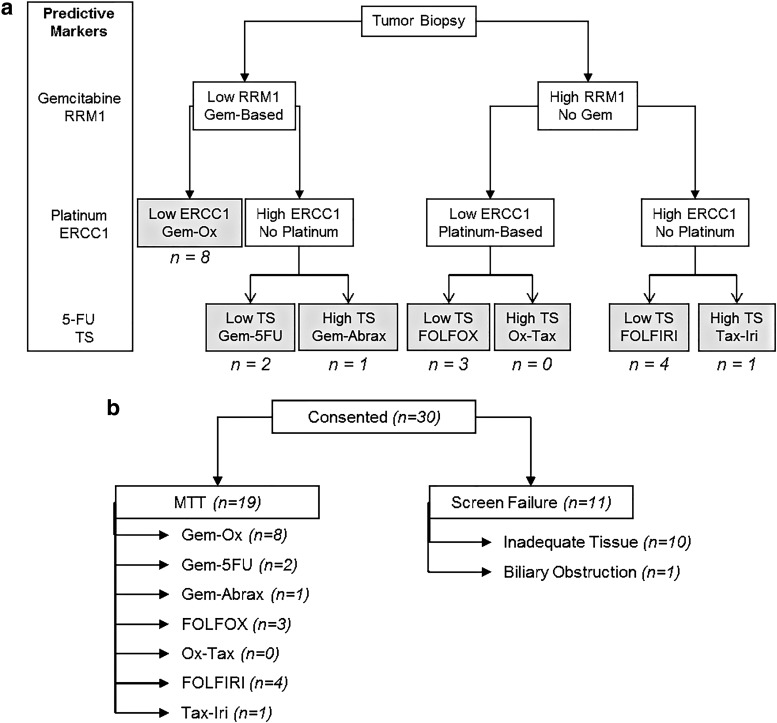
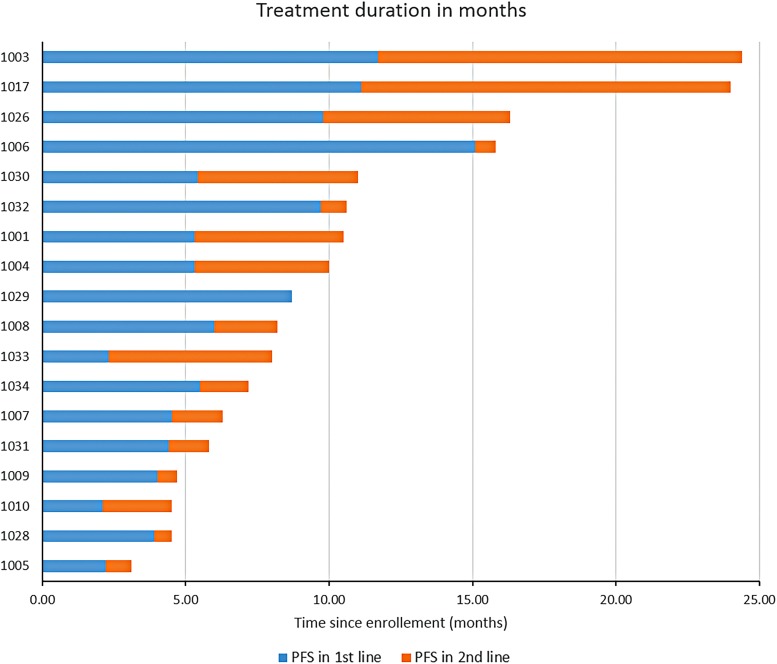
Despite the wide adoption of tumor molecular profiling, there is a dearth of evidence linking molecular biomarkers for treatment selection to prediction of treatment outcomes in patients with metastatic pancreatic cancer. We initiated a pilot study to test the feasibility of designing a larger phase II trial of molecularly tailored treatment for metastatic pancreatic cancer. Our study aimed to assess the feasibility of following a treatment algorithm based on the expression of three published predictive markers of response to chemotherapy: ribonucleotide reductase catalytic subunit M1 (for gemcitabine); excision repair cross-complementation group 1 (for platinum agents); and thymidylate synthase (for 5-fluorouracil) in patients with untreated, metastatic pancreatic cancer. Results of the tumor biopsy analysis were used to assign patients to one of seven doublet regimens. Key secondary objectives included response rate (RR), disease control rate (DCR), progression-free survival (PFS), and overall survival (OS). Between December 2012 and March 2015, 30 patients were enrolled into the study. Ten patients failed screening primarily due to inadequate tumor tissue availability. Of the remaining 20 patients, 19 were assigned into 6 different chemotherapy doublets, and achieved an RR of 28%, with a DCR rate of 78%. The median PFS and OS were 5.78 and 8.21 months, respectively. The incorporation of biomarkers into a treatment algorithm is feasible and resulted in a PFS and OS similar to other doublet therapies for patients with metastatic pancreatic cancer. Based on the results from this pilot study, a larger phase II randomized trial of molecularly targeted therapy versus physicians' choice of standard of care has been initiated in the second-line setting (NCT02967770).
尽管肿瘤分子谱分析已被广泛采用,但对于转移性胰腺癌患者,缺乏将用于治疗选择的分子生物标志物与治疗结果预测相关联的证据。我们开展了一项试点研究,以测试设计一项更大规模的转移性胰腺癌分子靶向治疗II期试验的可行性。我们的研究旨在评估在未经治疗的转移性胰腺癌患者中,根据三种已发表的化疗反应预测标志物的表达遵循治疗算法的可行性:核糖核苷酸还原酶催化亚基M1(针对吉西他滨);切除修复交叉互补组1(针对铂类药物);以及胸苷酸合成酶(针对5-氟尿嘧啶)。肿瘤活检分析结果用于将患者分配到七种双联方案之一。关键次要目标包括缓解率(RR)、疾病控制率(DCR)、无进展生存期(PFS)和总生存期(OS)。2012年12月至2015年3月期间,30名患者入组该研究。10名患者主要因肿瘤组织获取不足而筛查失败。在其余20名患者中,19名被分配到6种不同的化疗双联方案中,缓解率为28%,疾病控制率为78%。中位无进展生存期和总生存期分别为5.78个月和8.21个月。将生物标志物纳入治疗算法是可行的,并且对于转移性胰腺癌患者,其无进展生存期和总生存期与其他双联疗法相似。基于该试点研究的结果,已在二线治疗中启动了一项更大规模的分子靶向治疗与医生选择的标准治疗方案的II期随机试验(NCT02967770)。