Division of Cancer Prevention, National Cancer Institute, National Institutes of Health, Bethesda, Maryland.
Division of Cancer Epidemiology and Genetics, National Cancer Institute, National Institutes of Health, Bethesda, Maryland.
Cancer. 2019 Sep 1;125(17):2965-2974. doi: 10.1002/cncr.32176. Epub 2019 May 8.
The Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial assessed the effect of screening with prostate-specific antigen and a digital rectal examination on prostate cancer mortality. Another endpoint of interest was the burden of total metastatic disease.
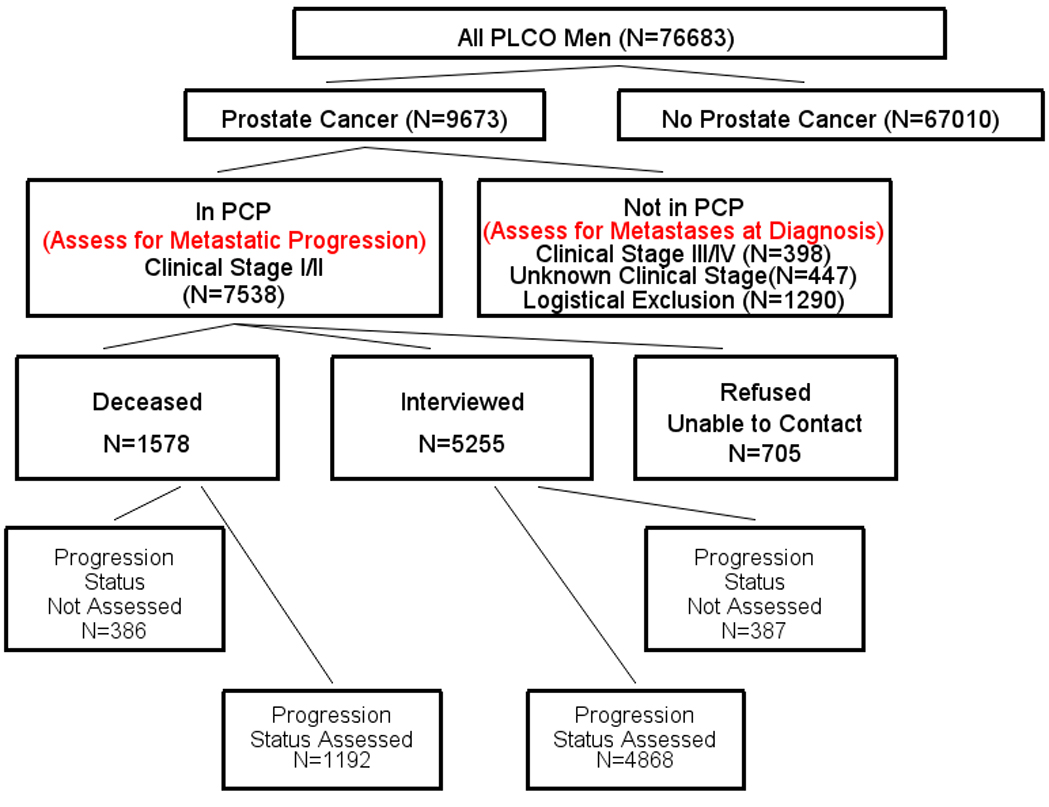
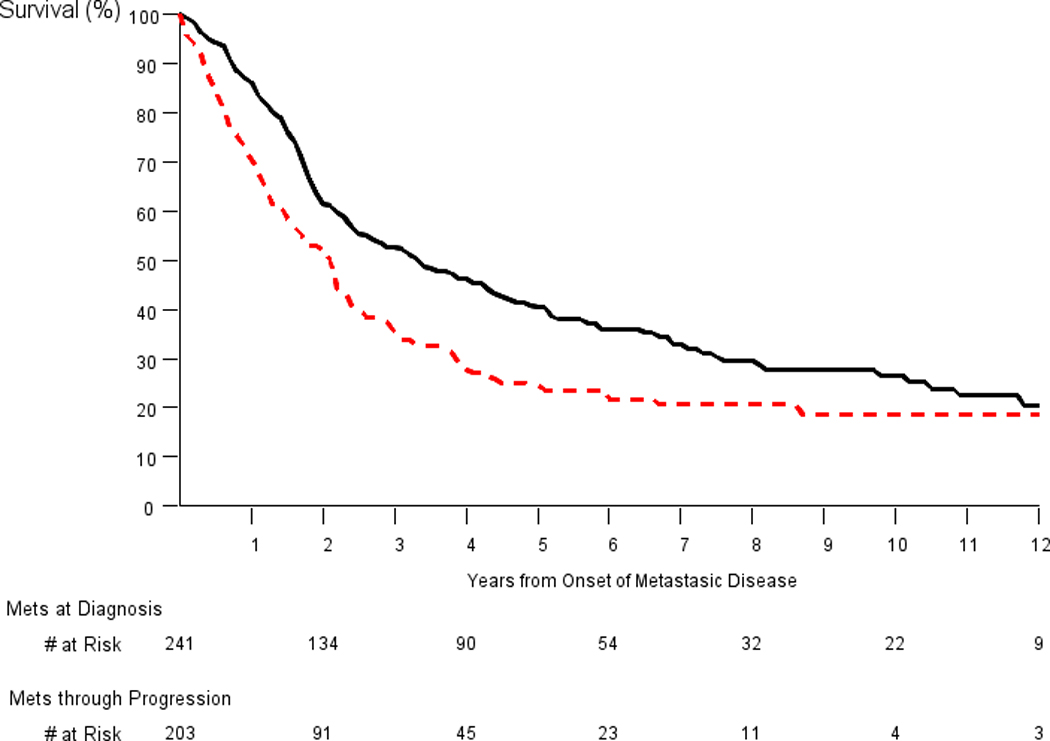
All men in PLCO were assessed for metastatic prostate cancer at diagnosis; men with clinical stage I/II disease were assessed for metastatic progression. The rate of total metastatic disease was defined as metastases found either at diagnosis or through progression divided by person-years (PYs) of follow-up for all men in the trial. Metastatic progression rates were computed among men with clinical stage I/II prostate cancer. Survival among men with metastases at diagnosis was compared with survival among men with metastatic progression.
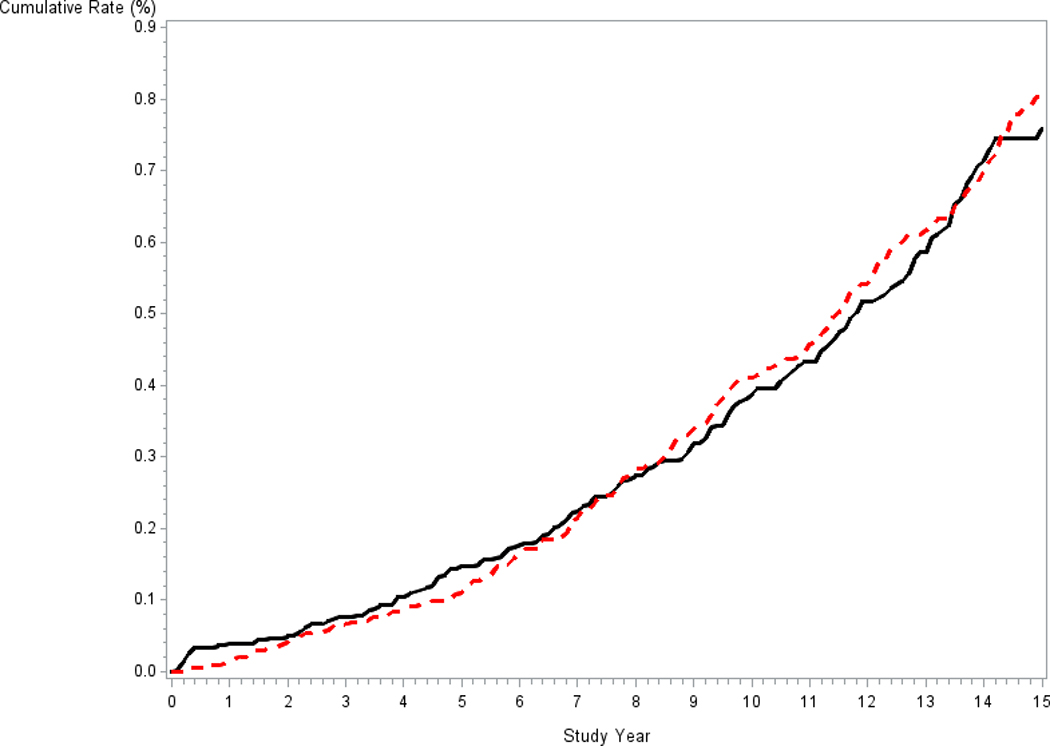
Among 38,340 men in the intervention arm and 38,343 men in the control arm in PLCO, there were 4974 and 4699 prostate cancer cases, respectively. The rates of total metastatic disease were 4.72 and 4.83 per 10,000 PYs in the intervention and control arms, respectively (rate ratio, 0.98; 95% CI, 0.81-1.18). The rates of metastatic progression among men with clinical stage I/II prostate cancer were 43.7 and 50.5 per 10,000 PYs in the intervention and control arms, respectively (P = .30). Prostate cancer-specific 5- and 10-year survival rates were significantly worse for men with metastatic progression (24% and 19%, respectively) than men with metastases at diagnosis (40% and 26%, respectively).
Rates of total metastatic disease and metastatic progression were similar across arms in PLCO. Survival was worse for men with metastatic progression in comparison with those with metastatic disease at diagnosis.
前列腺、肺、结直肠和卵巢(PLCO)癌症筛查试验评估了前列腺特异性抗原和数字直肠检查对前列腺癌死亡率的影响。另一个感兴趣的终点是总转移性疾病的负担。
PLCO 中的所有男性在诊断时都进行了转移性前列腺癌的评估;临床 I/II 期疾病的男性评估了转移性进展情况。总转移性疾病的发生率定义为在诊断时或通过进展发现的转移除以所有参与试验的男性的随访人年(PYs)。计算了临床 I/II 期前列腺癌男性的转移性进展率。在诊断时发生转移的男性的生存率与发生转移性进展的男性的生存率进行了比较。
在 PLCO 的干预组和对照组的 38340 名男性和 38343 名男性中,分别有 4974 例和 4699 例前列腺癌病例。干预组和对照组的总转移性疾病发生率分别为每 10000PYs 4.72 例和 4.83 例(比率为 0.98;95%CI,0.81-1.18)。临床 I/II 期前列腺癌男性的转移性进展率分别为干预组和对照组的每 10000PYs 43.7 例和 50.5 例(P=0.30)。转移性进展男性的前列腺癌特异性 5 年和 10 年生存率明显低于诊断时发生转移的男性(分别为 24%和 19%,分别为 40%和 26%)。
PLCO 各臂的总转移性疾病和转移性进展率相似。与诊断时发生转移性疾病的男性相比,转移性进展的男性的生存率更差。