Seo Veri, Baggett Travis P, Thorndike Anne N, Hull Peter, Hsu John, Newhouse Joseph P, Fung Vicki
Health Policy Research Center, Mongan Institute, Massachusetts General Hospital, 100 Cambridge Street, Ste. 1600, Boston, MA, 02114, USA.
Division of General Internal Medicine, Massachusetts General Hospital, 100 Cambridge St., Ste. 1600, Boston, MA, 02114, USA.
BMC Health Serv Res. 2019 May 8;19(1):291. doi: 10.1186/s12913-019-4124-z.
The Affordable Care Act expanded Medicaid and increased federal funding for Community Health Centers (CHCs). To examine the role of Medicaid coverage on care patterns for those with available safety net care, we assessed differences in access to care for CHC patients with continuous Medicaid coverage vs. gaps in insurance coverage in the last year.
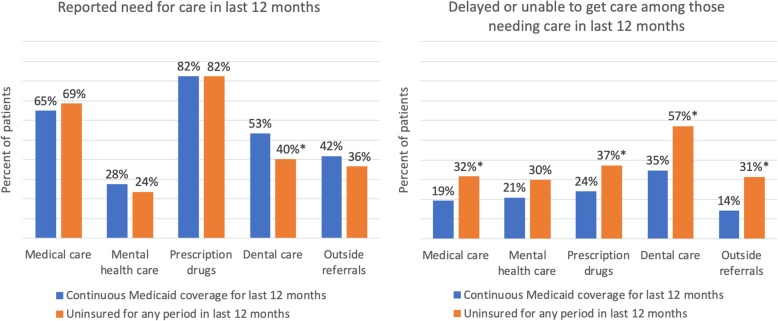
We used data on adult respondents from the 2014 Health Center Patient Survey (N = 1720) with continuous Medicaid coverage vs. those with some period without insurance coverage in the last 12 months. We examined reported need for any medical care, mental health care, prescription drugs, dental care, and referrals for care outside of the CHC in the last 12 months, and reports of being delayed or unable to get needed care by insurance status. We used logistic regression to assess the association between insurance status and care access, adjusting for patient characteristics.
Patients with insurance gaps and continuous Medicaid coverage reported similar levels of need for most types of care in the last 12 months, but those with insurance gaps were significantly more likely to report having difficulty obtaining medical care, prescription drugs, dental care, and completing outside referrals. Of those with incomplete referrals for care outside of the CHC, patients with insurance gaps were more likely than those with continuous Medicaid to cite cost or insurance-related reasons for not following up (70% vs. 19%, p < 0.01).
Having continuous Medicaid coverage appeared to mitigate barriers to care for CHC patients compared to having intermittent or no insurance coverage over the last year. Policies that increase disruptions in Medicaid coverage could adversely impact access to care, even among those with available safety net care.
《平价医疗法案》扩大了医疗补助范围,并增加了对社区卫生中心(CHC)的联邦资金投入。为了研究医疗补助覆盖对那些可获得安全网医疗服务者的就医模式的作用,我们评估了连续享有医疗补助的CHC患者与过去一年中存在保险覆盖缺口的患者在获得医疗服务方面的差异。
我们使用了2014年健康中心患者调查中成年受访者的数据(N = 1720),其中包括连续享有医疗补助的患者以及过去12个月内有一段时间无保险覆盖的患者。我们调查了过去12个月内报告的对任何医疗服务、心理健康服务、处方药、牙科护理以及转介至CHC以外机构接受治疗的需求,以及按保险状况报告的延迟或无法获得所需治疗的情况。我们使用逻辑回归来评估保险状况与获得医疗服务之间的关联,并对患者特征进行了调整。
有保险覆盖缺口的患者和连续享有医疗补助的患者在过去12个月内对大多数类型医疗服务的需求水平相似,但有保险覆盖缺口的患者更有可能报告在获得医疗服务、处方药、牙科护理以及完成外部转介方面存在困难。在那些未完成转介至CHC以外机构接受治疗的患者中,有保险覆盖缺口的患者比连续享有医疗补助的患者更有可能将费用或与保险相关的原因作为未跟进的理由(70%对19%,p < 0.01)。
与过去一年中间歇性或无保险覆盖相比,连续享有医疗补助似乎减轻了CHC患者获得医疗服务的障碍。增加医疗补助覆盖中断情况的政策可能会对获得医疗服务产生不利影响——即使是在那些可获得安全网医疗服务的人群中。