Department of Surgery, Division of Vascular Surgery, Radboud university medical center, Geert Grooteplein 10, Postbus 9101, 6500 HB, Nijmegen, the Netherlands.
Department of General Internal Medicine, Division of Vascular Medicine, Radboud university medical center, Nijmegen, the Netherlands.
BMC Med Res Methodol. 2019 May 9;19(1):95. doi: 10.1186/s12874-019-0743-7.
Poor medication adherence is a major factor in the secondary prevention of cardiovascular diseases (CVD) and contributes to increased morbidity, mortality, and costs. Interventions for improving medication adherence may have limited effects as a consequence of self selection of already highly adherent participants into clinical trials.
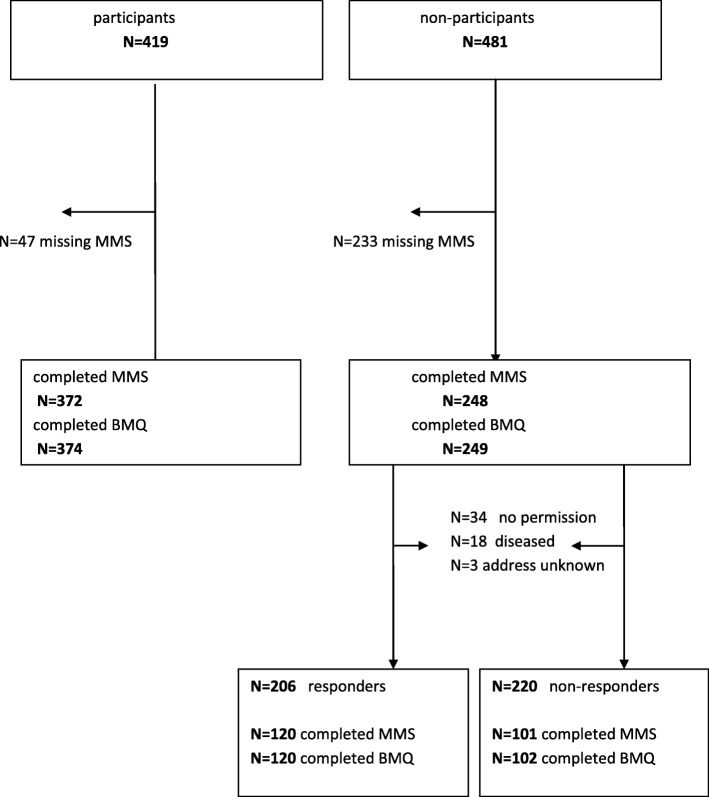
In this retrospective cohort study, existing levels of medication adherence were examined in self-decided participants and non-participants prior to inclusion in a randomized controlled study (RCT), evaluating the effect of an intervention to improve adherence. In addition, the non-participants were further divided into 'responders' and 'non responders'. All individuals had manifest cardiovascular disease and completed a questionnaire with baseline characteristics, the Beliefs about Medicines Questionnaire (BMQ) and the Modified Morisky Scale® (MMS®) as part of a regular screening program. A logistic regression was conducted to examine the relationship between study participation willingness, adherence level and the beliefs about medication.
According to the MMS® the adherence level was comparable in all groups. In both (non)-participants groups, 36% was classified as high adherent; 46% participants versus 44% non-participants were classified as medium adherent and 19% of the participants versus 20% of the non-participants were low adherent (p = 0.91. The necessity concern differential (NCD) from the BMQ was 3.8 for participants and 3.4 for non-participants (p = 0.32).
This study shows that adherence to medication and beliefs about medication do not differ between participants and non-participants before consenting to participate in an RCT. The study design seems not to have led to greater adherence in the study group.
药物依从性差是心血管疾病(CVD)二级预防的一个主要因素,导致发病率、死亡率和成本增加。改善药物依从性的干预措施的效果可能有限,因为临床试验已经将本来就高度依从的参与者自我选择纳入其中。
在这项回顾性队列研究中,在决定参加一项评估改善依从性干预效果的随机对照研究(RCT)之前,对自行决定参加和不参加研究的参与者的现有药物依从性水平进行了检查。此外,非参与者进一步分为“应答者”和“非应答者”。所有参与者均患有明显的心血管疾病,并完成了一份问卷,其中包括基线特征、药物信念问卷(BMQ)和改良 Morisky 量表®(MMS®),作为常规筛查计划的一部分。进行逻辑回归以检查研究参与意愿、依从水平和对药物的信念之间的关系。
根据 MMS®,所有组的依从水平相当。在(非)参与者组中,36%被归类为高依从;46%的参与者与 44%的非参与者被归类为中度依从,19%的参与者与 20%的非参与者被归类为低依从(p=0.91)。BMQ 的必要性关注差异(NCD)参与者为 3.8,非参与者为 3.4(p=0.32)。
这项研究表明,在同意参加 RCT 之前,参与者和非参与者的药物依从性和对药物的信念没有差异。研究设计似乎并没有导致研究组的依从性更高。