International Center for Circulatory Health, National Heart and Lung Institute, Imperial College London, Hammersmith Hospital, United Kingdom (T.W., C.M.C., J.P.H., Y.A., M.J.S.-S., R.P., S.S., S.N., R.A.L., D.P.F., J.E.D.).
Division of Cardiology, Department of Internal Medicine, St. Marianna University School of Medicine, Kawasaki, Japan (T.W., Y.I., Y.J.A.).
Circ Cardiovasc Interv. 2019 May;12(5):e007494. doi: 10.1161/CIRCINTERVENTIONS.118.007494.
Fractional flow reserve (FFR) and instantaneous wave-free ratio (iFR) disagree on the hemodynamic significance of a coronary lesion in ≈20% of cases. It is unknown whether the physiological pattern of disease is an influencing factor for this. This study assessed whether the physiological pattern of coronary artery disease influences discordance between FFR and iFR measurement.
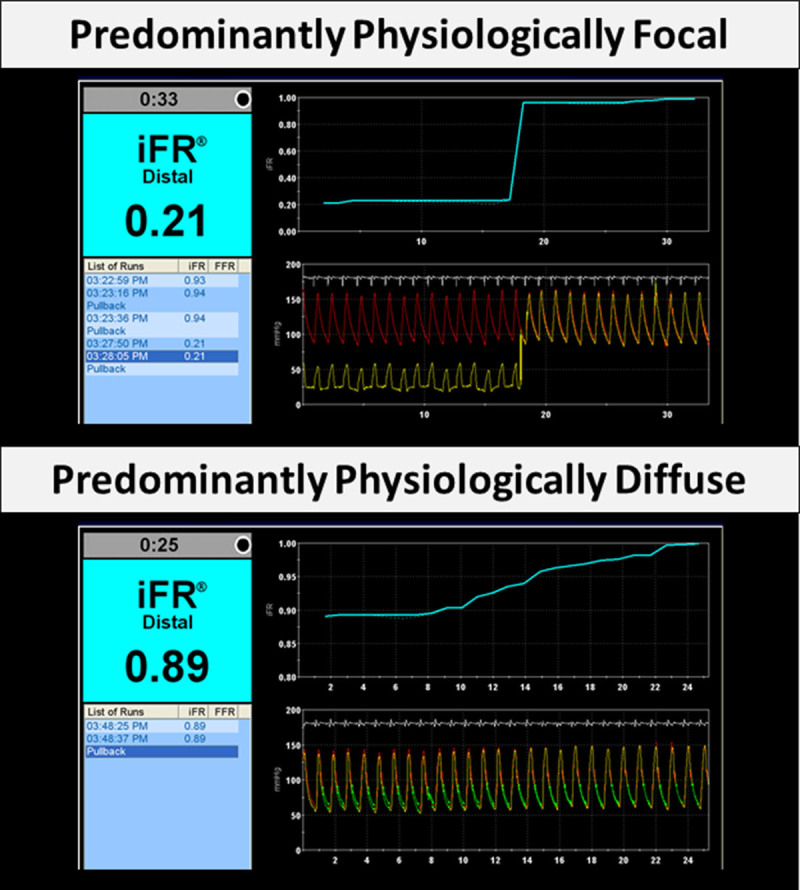
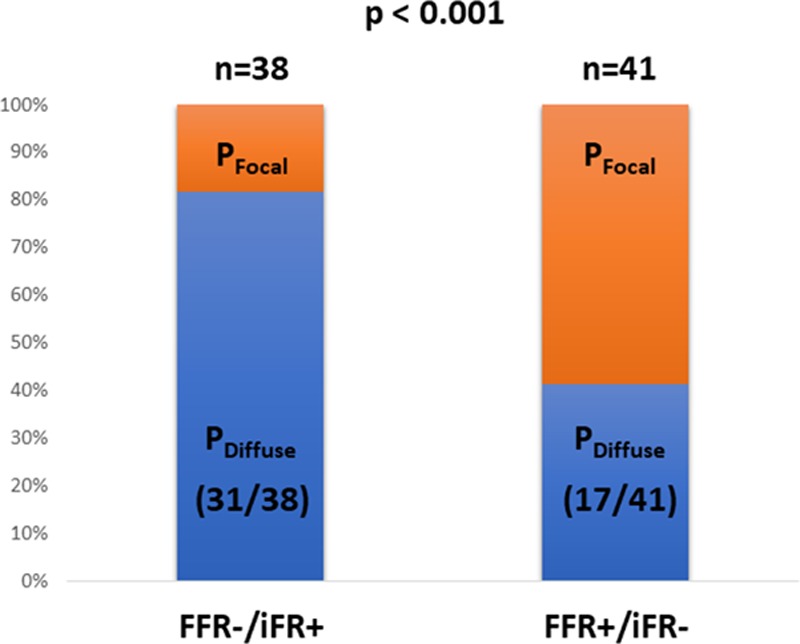
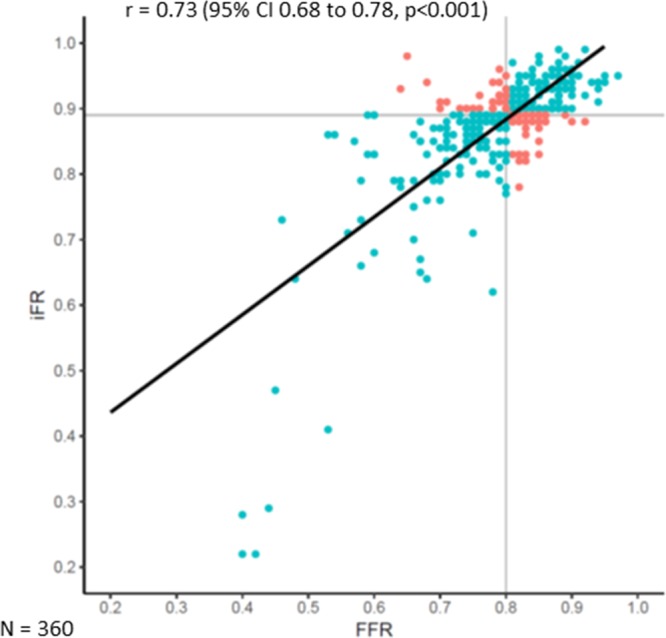
Three-hundred and sixty intermediate coronary lesions (345 patients; mean age, 64.4±10.3 years; 76% men) with combined FFR, iFR, and iFR pressure-wire pullback were included for analysis from an international multicenter registry. Cut points for hemodynamic significance were FFR ≤0.80 and iFR ≤0.89, respectively. Lesions were classified into FFR+/iFR+ (n=154; 42.7%), FFR-/iFR+ (n=38; 10.6%), FFR+/iFR- (n=41; 11.4%), and FFR-/iFR- (n=127; 35.3%) groups. The physiological pattern of disease was classified according to the iFR pullback recordings as predominantly physiologically focal (n=171; 47.5%) or predominantly physiologically diffuse (n=189; 52.5%). Median FFR and iFR were 0.80 (interquartile range, 0.75-0.85) and 0.89 (interquartile range, 0.86-0.92), respectively. FFR disagreed with iFR in 22% (79 of 360). The physiological pattern of disease was the only influencing factor relating to FFR/iFR discordance: predominantly physiologically focal was significantly associated with FFR+/iFR- (58.5% [24 of 41]), and predominantly physiologically diffuse was significantly associated with FFR-/iFR+ (81.6% [31 of 38]; P<0.001 for pattern of disease between FFR+/iFR- and FFR-/iFR+ groups).
The physiological pattern of coronary artery disease was an important influencing factor for FFR/iFR discordance.
在约 20%的病例中,血流储备分数(FFR)和瞬时无波比(iFR)对冠状动脉病变的血流动力学意义存在分歧。目前尚不清楚疾病的生理模式是否是影响这一分歧的一个因素。本研究评估了冠状动脉疾病的生理模式是否会影响 FFR 和 iFR 测量之间的不匹配。
本研究纳入了来自国际多中心注册研究的 360 处中等程度的冠状动脉病变(345 例患者;平均年龄 64.4±10.3 岁;76%为男性),这些病变均进行了 FFR、iFR 和 iFR 压力导丝回撤的联合检测。血流动力学意义的截断值分别为 FFR≤0.80 和 iFR≤0.89。病变分为 FFR+/iFR+(n=154;42.7%)、FFR-/iFR+(n=38;10.6%)、FFR+/iFR-(n=41;11.4%)和 FFR-/iFR-(n=127;35.3%)组。根据 iFR 回撤记录,将病变的生理模式分为主要为生理性局灶性(n=171;47.5%)或主要为生理性弥漫性(n=189;52.5%)。中位 FFR 和 iFR 分别为 0.80(四分位距 0.75-0.85)和 0.89(四分位距 0.86-0.92)。FFR 与 iFR 不匹配的比例为 22%(79/360)。疾病的生理模式是唯一与 FFR/iFR 不匹配相关的影响因素:主要为生理性局灶性与 FFR+/iFR-(58.5%[24/41])显著相关,主要为生理性弥漫性与 FFR-/iFR+(81.6%[31/38])显著相关(FFR+/iFR-与 FFR-/iFR+组之间的疾病模式差异具有统计学意义,P<0.001)。
冠状动脉疾病的生理模式是 FFR/iFR 不匹配的一个重要影响因素。