Bayer AG, Market Access, Pharmaceuticals, Berlin, Germany.
IQVIA Commercial GmbH & Co. OHG, Unterschweinstiege 2-14, 60549, Frankfurt/Main, Germany.
BMC Nephrol. 2019 May 16;20(1):171. doi: 10.1186/s12882-019-1348-4.
Steroidal mineralocorticoid receptor antagonists (MRAs) are recommended for the treatment of heart failure (HF) and resistant hypertension, both common comorbidities in patients with diabetes and chronic kidney disease (CKD). This study explored the clinical characteristics of, and steroidal MRA use in, patients with CKD with and without type 2 diabetes mellitus (T2D) and/or HF.
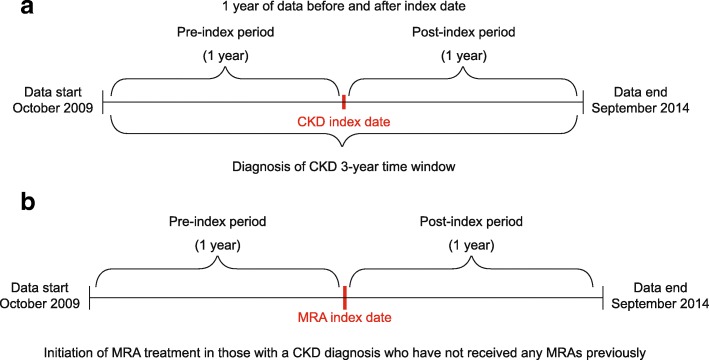
This retrospective cohort study used PharMetrics Plus US claims database data (October 2009-September 2014) to identify two patient populations aged ≥18 years with a first diagnosis of CKD or a first prescription for steroidal MRAs. Demographic characteristics, comorbidities, clinical events, medication use and healthcare costs were reported by population and stratified by diagnosis: CKD, CKD + T2D (DKD), CKD + HF and DKD + HF. The CKD population cohorts were further stratified by steroidal MRA treatment duration (no MRAs, < 6 and ≥ 6 months' treatment).
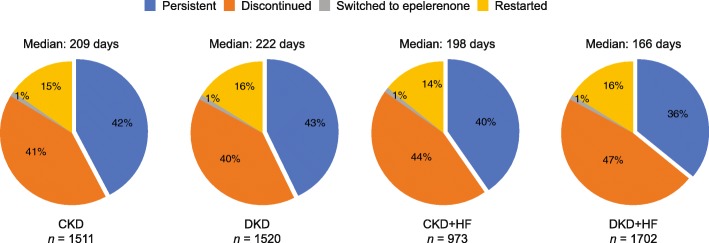
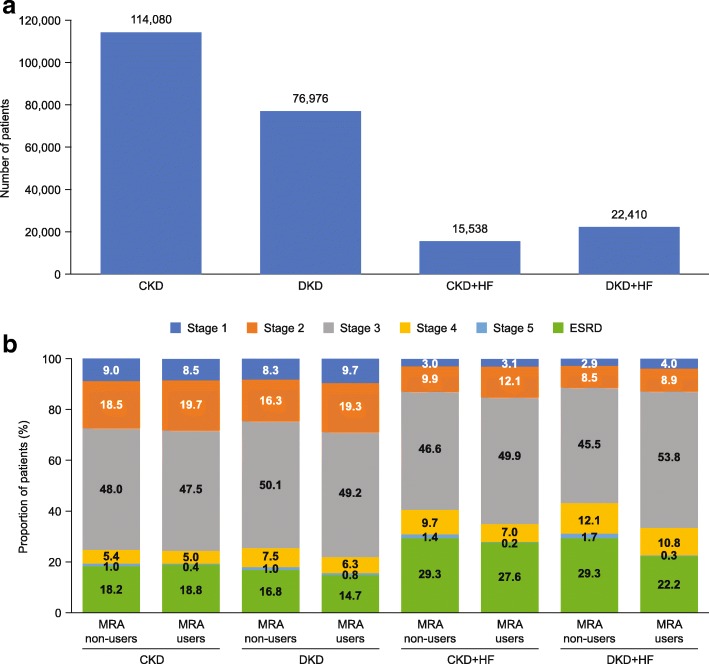
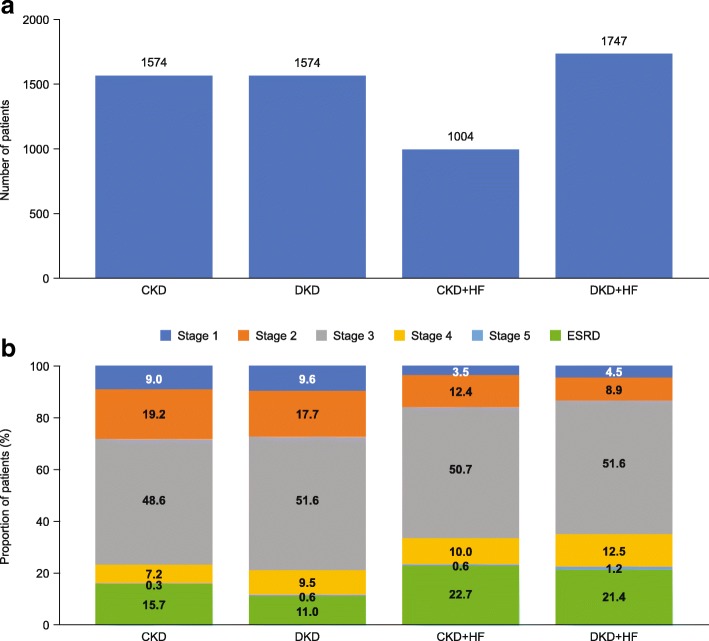
The CKD and MRA populations comprised 229,004 patients and 5899 patients, respectively. Median age and the proportion of men were similar in the CKD and MRA populations across disease cohorts. Disease burden increased across the cohorts as comorbidity and clinical event incidences increased. Hypertension was reported in 70-92% of patients, irrespective of disease cohort or population. In the CKD population, MRA use was low but increased with disease burden: CKD, 1.2%; DKD, 1.8%; CKD + HF, 6.5%; and DKD + HF, 6.6%. Moreover, MRA users presented with higher rates of comorbidities and medication use, and higher healthcare costs than MRA non-users. Longer MRA treatment duration was associated with reduced polypharmacy, lower event rates and lower healthcare costs. In the MRA population, patients almost exclusively received spironolactone (≥ 96%; median dose across all groups 25 mg; one-year persistence, ≤ 43%); up to 16% of patients had end-stage renal disease at baseline despite steroidal MRAs being contraindicated.
Steroidal MRA use was low across all cohorts, but increased with disease severity, driven particularly by HF. Steroidal MRAs were used in patients with advanced CKD, despite being contraindicated. The persistent morbidity and clinical event rates in CKD and DKD patients highlight the disease burden and the need for treatments that effectively target both cardio-vascular and kidney-related events.
甾体制剂盐皮质激素受体拮抗剂(MRAs)被推荐用于治疗心力衰竭(HF)和耐药性高血压,这两种疾病都是糖尿病和慢性肾脏病(CKD)患者常见的合并症。本研究探讨了伴有和不伴有 2 型糖尿病(T2D)和/或 HF 的 CKD 患者的临床特征和甾体制剂 MRA 的使用情况。
本回顾性队列研究使用 PharMetrics Plus US 索赔数据库数据(2009 年 10 月至 2014 年 9 月),确定了两个年龄≥18 岁的患者人群,他们的首次诊断为 CKD 或首次处方甾体制剂 MRA。按人群报告人口统计学特征、合并症、临床事件、药物使用和医疗保健费用,并按诊断分层:CKD、CKD+T2D(DKD)、CKD+HF 和 DKD+HF。CKD 患者人群进一步按甾体制剂 MRA 治疗时间(无 MRA、<6 个月和≥6 个月)分层。
CKD 和 MRA 患者人群分别包括 229004 名患者和 5899 名患者。在疾病队列中,CKD 和 MRA 患者的中位年龄和男性比例相似。随着合并症和临床事件发生率的增加,疾病负担在各队列中增加。高血压的报告率在 70-92%的患者中,无论疾病队列或人群如何。在 CKD 患者中,MRA 的使用率较低,但随着疾病负担的增加而增加:CKD,1.2%;DKD,1.8%;CKD+HF,6.5%;DKD+HF,6.6%。此外,MRA 使用者的合并症和药物使用频率更高,医疗保健费用也更高。较长的 MRA 治疗时间与减少多种药物治疗、降低事件发生率和降低医疗保健费用相关。在 MRA 患者人群中,几乎所有患者(≥96%)均接受螺内酯治疗(所有组的中位剂量均为 25mg;一年的持续率,≤43%);尽管甾体制剂 MRA 是禁忌的,但基线时有多达 16%的患者患有终末期肾病。
在所有队列中,MRA 的使用率都较低,但随着疾病严重程度的增加而增加,尤其是与 HF 有关。甾体制剂 MRA 被用于患有晚期 CKD 的患者,尽管存在禁忌证。CKD 和 DKD 患者的持续发病率和临床事件发生率突出了疾病负担以及需要有效的治疗方法来靶向心血管和肾脏相关事件的必要性。