Indiana University School of Medicine and VA Medical Center, 1481 West 10th Street, 111N Indianapolis, IN 46202, USA.
R&D Preclinical Research Cardiovascular, Bayer AG, Wuppertal, Germany.
Eur Heart J. 2021 Jan 7;42(2):152-161. doi: 10.1093/eurheartj/ehaa736.
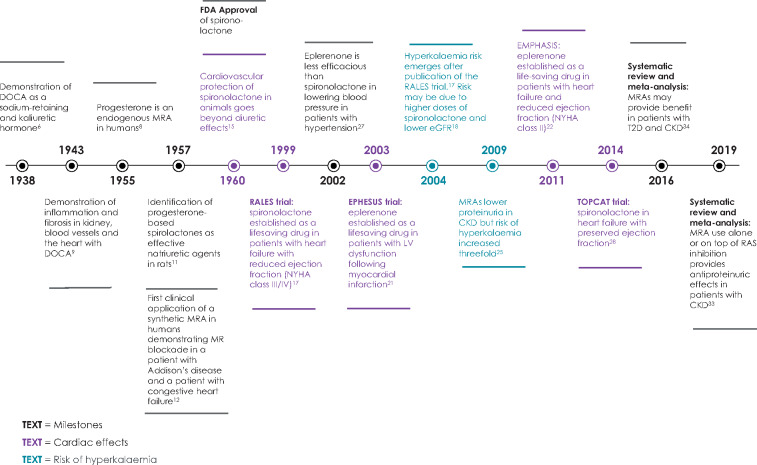
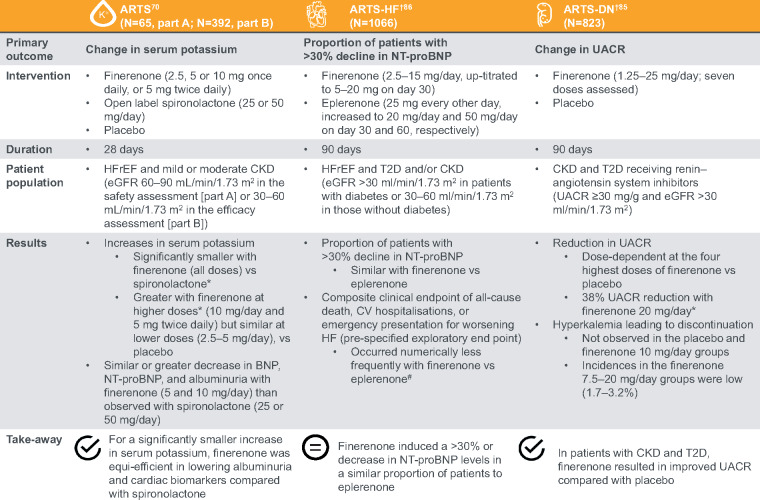
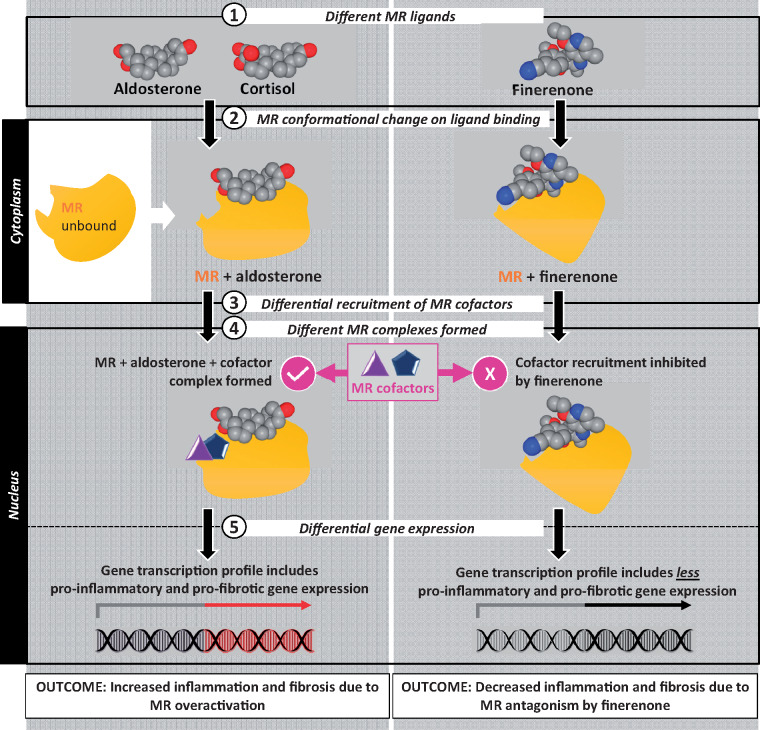
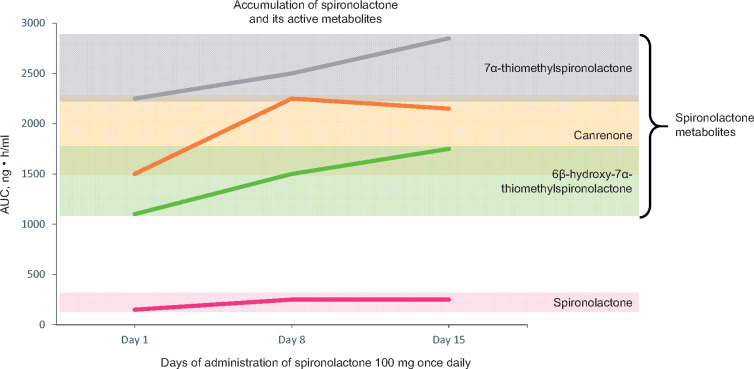
This review covers the last 80 years of remarkable progress in the development of mineralocorticoid receptor (MR) antagonists (MRAs) from synthesis of the first mineralocorticoid to trials of nonsteroidal MRAs. The MR is a nuclear receptor expressed in many tissues/cell types including the kidney, heart, immune cells, and fibroblasts. The MR directly affects target gene expression-primarily fluid, electrolyte and haemodynamic homeostasis, and also, but less appreciated, tissue remodelling. Pathophysiological overactivation of the MR leads to inflammation and fibrosis in cardiorenal disease. We discuss the mechanisms of action of nonsteroidal MRAs and how they differ from steroidal MRAs. Nonsteroidal MRAs have demonstrated important differences in their distribution, binding mode to the MR and subsequent gene expression. For example, the novel nonsteroidal MRA finerenone has a balanced distribution between the heart and kidney compared with spironolactone, which is preferentially concentrated in the kidneys. Compared with eplerenone, equinatriuretic doses of finerenone show more potent anti-inflammatory and anti-fibrotic effects on the kidney in rodent models. Overall, nonsteroidal MRAs appear to demonstrate a better benefit-risk ratio than steroidal MRAs, where risk is measured as the propensity for hyperkalaemia. Among patients with Type 2 diabetes, several Phase II studies of finerenone show promising results, supporting benefits on the heart and kidneys. Furthermore, finerenone significantly reduced the combined primary endpoint (chronic kidney disease progression, kidney failure, or kidney death) vs. placebo when added to the standard of care in a large Phase III trial.
这篇综述涵盖了过去 80 年来,在开发盐皮质激素受体(MR)拮抗剂(MRA)方面的显著进展,从第一类盐皮质激素的合成到非甾体类 MRA 的临床试验。MR 是一种在许多组织/细胞类型中表达的核受体,包括肾脏、心脏、免疫细胞和成纤维细胞。MR 直接影响靶基因的表达,主要是体液、电解质和血液动力学的稳态,也但不太被重视,是组织重塑。MR 的病理生理过度激活导致心脏肾脏疾病中的炎症和纤维化。我们讨论了非甾体类 MRA 的作用机制,以及它们与甾体类 MRA 的区别。非甾体类 MRA 在其分布、与 MR 的结合模式以及随后的基因表达方面表现出重要差异。例如,新型非甾体类 MRA 非奈利酮与螺内酯相比,在心脏和肾脏之间的分布更为平衡,而螺内酯则优先集中在肾脏。与依普利酮相比,非奈利酮在啮齿动物模型中显示出更强的抗炎和抗纤维化作用,等效于依普利酮的剂量。总的来说,非甾体类 MRA 似乎比甾体类 MRA 具有更好的获益风险比,风险是指高钾血症的倾向。在 2 型糖尿病患者中,几项非奈利酮的 II 期研究显示出有前景的结果,支持对心脏和肾脏的益处。此外,非奈利酮与标准治疗联合应用时,在一项大型 III 期试验中显著降低了主要复合终点(慢性肾脏病进展、肾衰竭或肾脏死亡)的发生率,与安慰剂相比。