Department of Community Health Sciences, Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada.
Department of Cancer Epidemiology and Prevention Research, CancerControl Alberta, Alberta Health Services, Calgary, Alberta, Canada.
JAMA Netw Open. 2019 May 3;2(5):e194154. doi: 10.1001/jamanetworkopen.2019.4154.
The results from the recent International Duration Evaluation of Adjuvant Therapy (IDEA) collaboration have led some clinicians to adopt shorter durations of adjuvant chemotherapy for patients with stage III colon cancer. The extent to which these findings are supported by other data is unknown.
To conduct a systematic review and meta-analysis of randomized and observational studies investigating the association between the duration of adjuvant chemotherapy and survival among individuals diagnosed as having stage II and III colon cancer (PROSPERO protocol CRD42018108711]).
Abstracts published in English between 2003 and 2018 within the MEDLINE, Embase, CENTRAL, and CINAHL databases were reviewed by 2 authors. Also searched were conference proceedings and the indexes of high-impact oncology journals.
Studies were excluded if they did not present original data; focused on animal populations, on cancers in sites other than the colon, or on patients with stage 0, I, or IV disease; did not examine a 5-flourouracil-based monotherapy or combination therapy; or did not evaluate the association between treatment duration and survival. The search identified 2341 articles, from which 2 randomized trials and 20 observational studies were included in the meta-analysis.
This study followed the PRISMA and MOOSE reporting guidelines. The risk of bias was assessed by 2 authors using the Cochrane and Risk of Bias in Nonrandomized Studies of Interventions (ROBINS-I) tools. The results were synthesized using a random-effects model.
The primary and secondary outcomes were overall survival and disease-free survival, respectively. It was hypothesized a priori that 3 months of chemotherapy would be as effective as 6 months of chemotherapy.
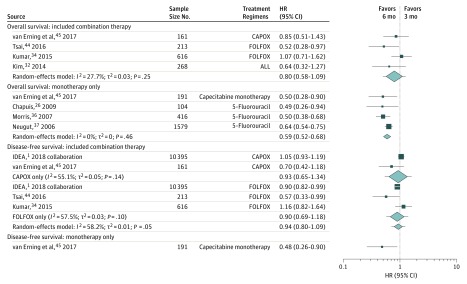
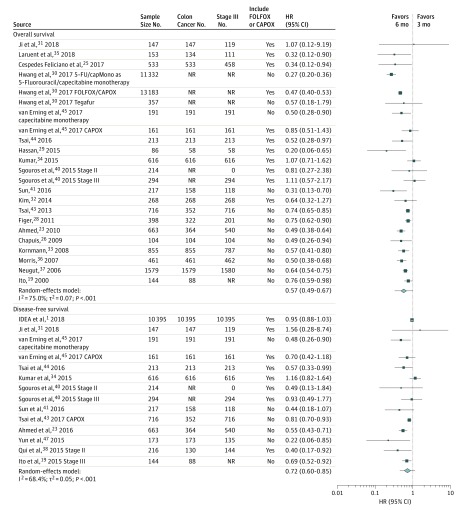
Twenty-two studies were included in the meta-analysis, representing 43 671 patients. The inclusion of patients with stage II disease or with rectal cancer was identified as a source of heterogeneity. After restricting the analysis to patients with stage III colon cancer, there was no association between the duration of chemotherapy and overall survival among studies involving FOLFOX (leucovorin calcium [folinic acid], fluorouracil, and oxaliplatin) or CAPOX (capecitabine plus oxaliplatin) regimens (hazard ratio [HR], 0.80; 95% CI, 0.58-1.09). Among studies focused exclusively on monotherapy, the standard 6-month regimen relative to a 3-month regimen was associated with improved survival (HR, 0.59; 95% CI, 0.52-0.68).
Shortened durations of chemotherapy may reduce survival among patients with stage III colon cancer prescribed monotherapy but not a combination regimen.
最近国际辅助治疗持续时间评估 (IDEA) 合作的结果导致一些临床医生为 III 期结肠癌患者采用更短的辅助化疗持续时间。这些发现得到其他数据支持的程度尚不清楚。
对随机和观察性研究进行系统评价和荟萃分析,以调查辅助化疗持续时间与 II 期和 III 期结肠癌(PROSPERO 方案 CRD42018108711])诊断的个体生存之间的关联。
2 位作者对 2003 年至 2018 年间在 MEDLINE、Embase、CENTRAL 和 CINAHL 数据库中以英文发表的摘要进行了审查。还检索了会议记录和高影响力肿瘤学杂志的索引。
如果研究没有提供原始数据;重点是动物群体、结外部位的癌症或 0、I 或 IV 期疾病的患者;未检查 5-氟尿嘧啶为基础的单药或联合治疗;或未评估治疗持续时间与生存之间的关系,则排除研究。该搜索确定了 2341 篇文章,其中 2 项随机试验和 20 项观察性研究被纳入荟萃分析。
本研究遵循 PRISMA 和 MOOSE 报告指南。2 位作者使用 Cochrane 和非随机干预研究的风险偏倚工具 (ROBINS-I) 评估了风险偏倚。使用随机效应模型综合结果。
主要和次要结果分别是总生存和无病生存。假设化疗 3 个月与化疗 6 个月一样有效。
荟萃分析包括 22 项研究,代表 43671 名患者。确定纳入 II 期疾病或直肠癌患者是异质性的一个来源。在将分析仅限于 III 期结肠癌患者后,FOLFOX(亚叶酸钙[叶酸]、氟尿嘧啶和奥沙利铂)或 CAPOX(卡培他滨加奥沙利铂)方案的研究中,化疗持续时间与总生存之间没有关联(风险比 [HR],0.80;95%CI,0.58-1.09)。在专门针对单药治疗的研究中,与标准 6 个月方案相比,3 个月方案与生存改善相关(HR,0.59;95%CI,0.52-0.68)。
缩短化疗持续时间可能会降低接受单药治疗而非联合方案治疗的 III 期结肠癌患者的生存。