Department of Hematology Oncology, Indiana University School of Medicine, 535 Barnhill Drive, RT 473, Indianapolis, IN, 46202, USA.
Department of Biostatistics-HS3000, Indiana University School of Medicine, 410 West 10th; Street, Indianapolis, IN, 46202, USA.
BMC Cancer. 2019 May 17;19(1):468. doi: 10.1186/s12885-019-5630-4.
Only a few patients with pancreatic ductal adenocarcinoma (PDAC) recurring after curative resection and peri-operative (neoadjuvant and adjuvant) therapy are included in clinical trials of metastatic PDAC. As such, there is a paucity of data to guide treatment after relapse, and patients are treated similarly to those with de novo metastatic PDAC (mPDAC). We evaluated the patterns of chemotherapy use and over-all survival (OS) in patients with recurrent PDAC (rPDAC) following curative therapy.
In this retrospective study, the Indiana University pancreatic cancer database was used to identify patients with PDAC who underwent curative resection and subsequently developed recurrence. Demographics, tumor and treatment characteristics were collected. Patients were broadly divided into those who received chemotherapy for rPDAC and those who did not. Patients in the former category were further subdivided into those who received single agent therapy, any standard combination therapy (5-fluorouracil/irinotecan/oxaliplatin combination or gemcitabine/nab-paclitaxel) and those who received non-standard combinations. Survival analysis was performed by the Kaplan-Meier method. Log rank tests were used to determine differences in survival between treated rPDAC patients and those not treated. Cox regression analysis was employed to evaluate factors associated with OS.
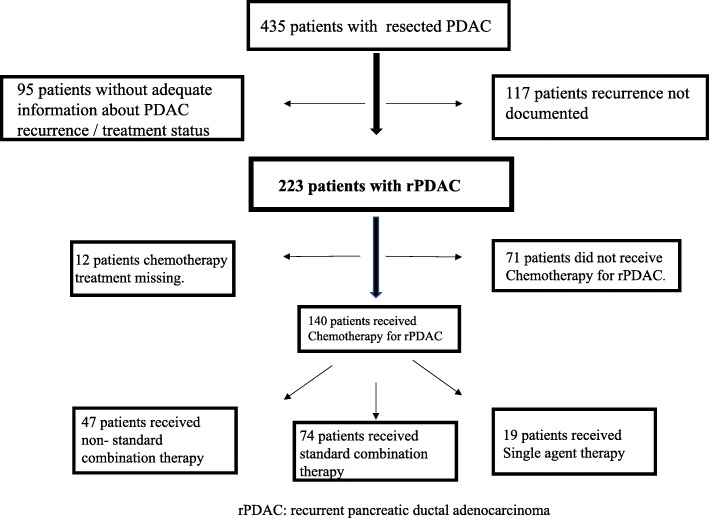
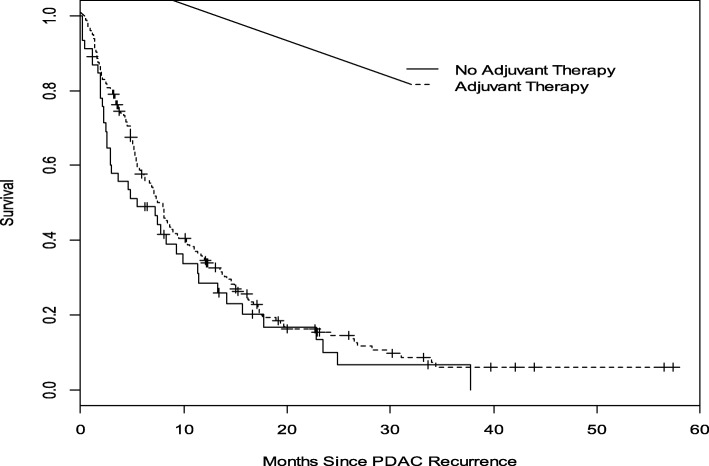
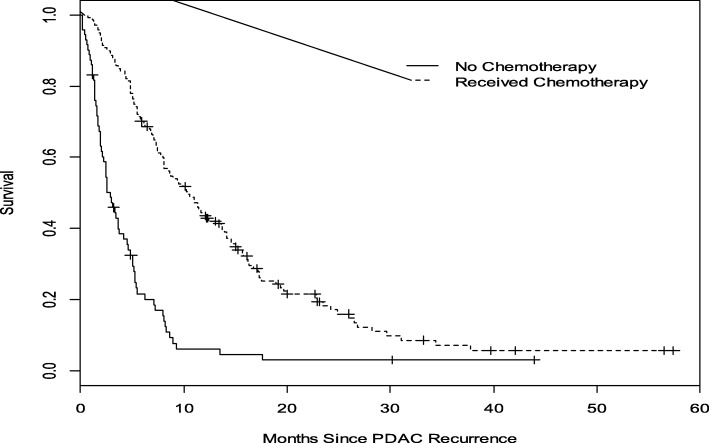
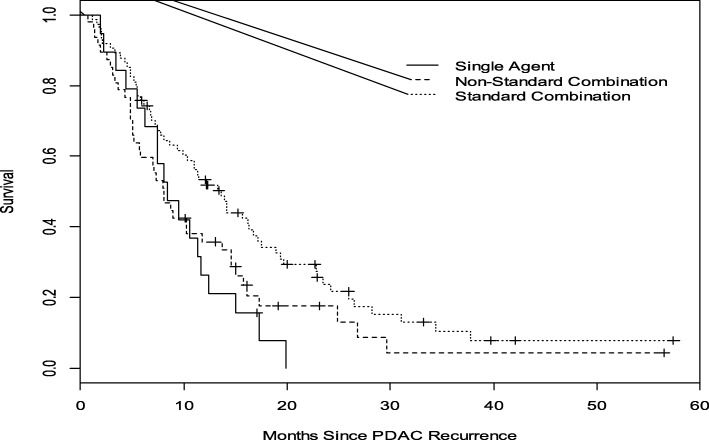
We identified 435 patients with resected PDAC treated between 2008 and 2014. Two hundred and twenty-three patients (51.2%) were diagnosed with rPDAC. Of these, 140 patients (63%) received chemotherapy whereas 71 patients (32%) did not receive chemotherapy. The 74 patients (53%) who received any standard, approved multiagent combination regimen had a median OS of 14 months compared to 8 months for the 47 patents (34%) who received other non-standard combinations and the 19 (13%) who received single agent therapy (P = 0.029). Multivariate cox regression analysis showed that margin negative resection, peri-operative therapy, radiotherapy and the use of any chemotherapy for rPDAC were associated with improved OS.
Our findings support the use of standard approved multi-agent therapy in rPDAC. Patients derive significant benefit from these standard combination therapies with median OS that is comparable to what is observed with treatment for de novo mPDAC.
只有少数接受根治性切除术和围手术期(新辅助和辅助)治疗后复发的胰腺导管腺癌(PDAC)患者被纳入转移性 PDAC 的临床试验。因此,缺乏指导复发后治疗的数据,并且这些患者的治疗方法与新发转移性 PDAC(mPDAC)患者相似。我们评估了根治性治疗后复发 PDAC(rPDAC)患者的化疗使用模式和总生存期(OS)。
在这项回顾性研究中,印第安纳大学胰腺癌数据库被用于确定接受根治性切除术并随后发生复发的 PDAC 患者。收集了人口统计学、肿瘤和治疗特征。患者大致分为接受 rPDAC 化疗的患者和未接受化疗的患者。前者进一步分为接受单药治疗、任何标准联合治疗(5-氟尿嘧啶/伊立替康/奥沙利铂联合或吉西他滨/白蛋白紫杉醇)和接受非标准联合治疗的患者。采用 Kaplan-Meier 法进行生存分析。对数秩检验用于确定治疗 rPDAC 患者和未治疗患者之间的生存差异。Cox 回归分析用于评估与 OS 相关的因素。
我们确定了 435 名 2008 年至 2014 年接受根治性 PDAC 治疗的患者。其中 223 名(51.2%)患者被诊断为 rPDAC。在这些患者中,140 名(63%)接受了化疗,而 71 名(32%)未接受化疗。74 名(53%)接受任何标准批准的多药联合方案治疗的患者中位 OS 为 14 个月,而 47 名(34%)接受其他非标准联合治疗的患者和 19 名(13%)接受单药治疗的患者中位 OS 为 8 个月(P=0.029)。多因素 Cox 回归分析显示,阴性切缘切除术、围手术期治疗、放疗和 rPDAC 的任何化疗的使用与 OS 改善相关。
我们的研究结果支持在 rPDAC 中使用标准批准的多药联合治疗。这些标准联合治疗可显著改善患者的生存获益,中位 OS 与治疗新发 mPDAC 相当。