Department of Clinical Pharmacy, University Medical Center Utrecht, PO Box 85500, 3508 GA, Utrecht, The Netherlands.
Department of Clinical Pharmacy, Meander Medical Center, Amersfoort, The Netherlands.
Clin Pharmacokinet. 2019 Aug;58(8):1069-1075. doi: 10.1007/s40262-019-00744-6.
During inflammation, elevated total (unbound plus protein-bound) clozapine plasma concentrations have been observed. Elevated alpha-1-acid glycoprotein concentrations during inflammation are suggested to cause increased plasma clozapine-alpha-1-acid glycoprotein binding, resulting in elevated total clozapine plasma concentrations without significant changes in unbound concentrations. Here, we investigated the association between alpha-1-acid glycoprotein plasma concentrations and clozapine unbound fraction.
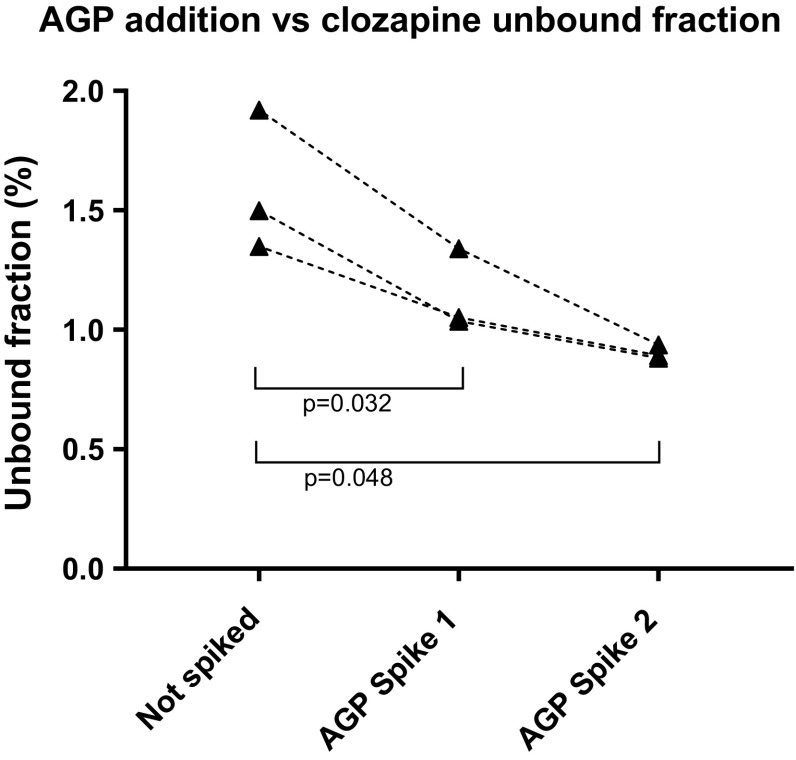
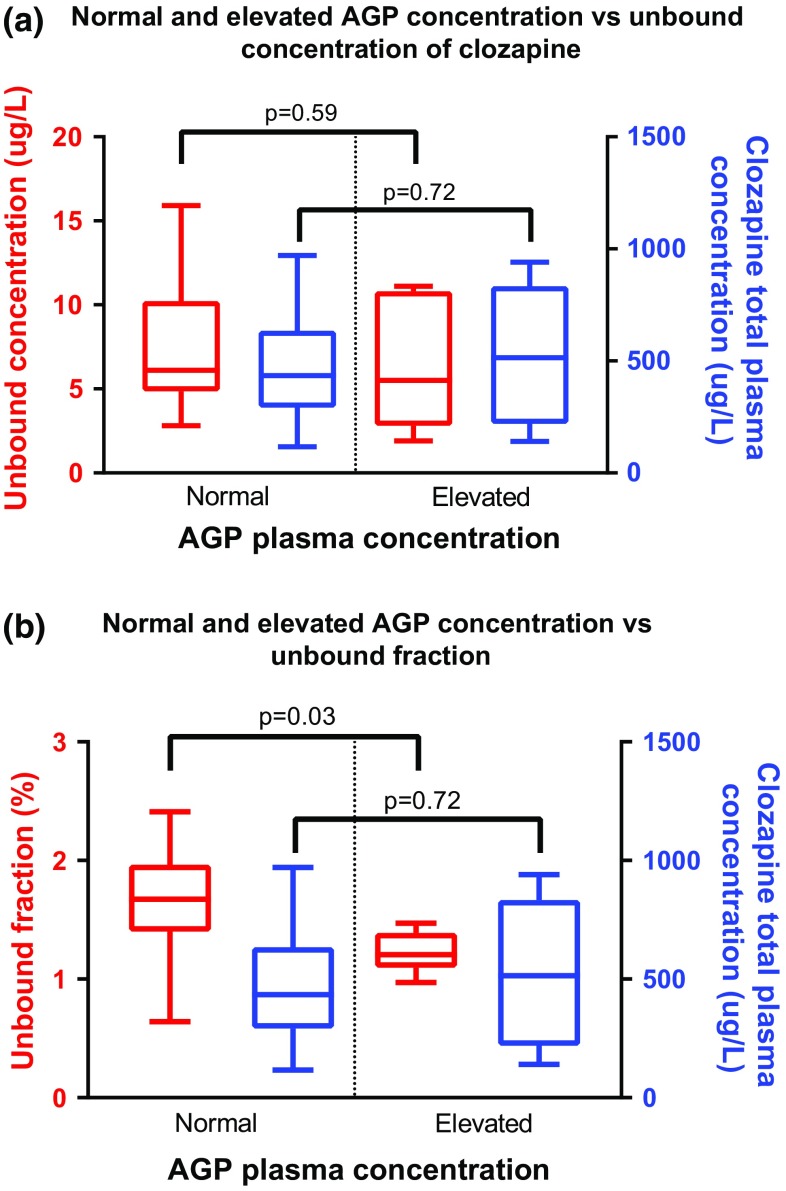
First, 25 and 60 µL of alpha-1-acid glycoprotein solution (20 mg/mL) were added to plasma samples (n = 3) of clozapine users (spiking experiment). Second, the association between alpha-1-acid glycoprotein plasma concentration and clozapine unbound fraction was assessed in patient samples (patient study). Samples were determined by liquid chromatography-tandem mass spectrometry. Data were analyzed with a paired t test (spiking experiment) and an unpaired t test (patient study).
The spiking experiment showed significantly lower mean unbound fractions following 25- and 60-µL alpha-1-acid glycoprotein spikes (relative reductions of 28.3%, p = 0.032 and 43.4%, p = 0.048). In the patient study, total clozapine plasma concentrations were 10% higher in elevated (n = 6) compared with normal alpha-1-acid glycoprotein (n = 20) samples [525 µg/L vs. 479 µg/L, mean difference = 47 µg/L (95% confidence interval -217 to 310), p = 0.72]. Elevated alpha-1-acid glycoprotein samples had a 26% lower mean unbound fraction compared with normal samples [1.22% vs. 1.65%, mean difference = -0.43% (95% confidence interval -0.816 to -0.0443), p = 0.03].
Both the spiking experiment and patient study showed a significant association between elevated alpha-1-acid glycoprotein plasma concentrations and a lower clozapine unbound fraction. Future studies should include clinical data to examine whether this association is clinically relevant, suggesting any clozapine dose adjustments.
在炎症期间,观察到总(未结合蛋白结合的)氯氮平血浆浓度升高。炎症期间α-1-酸性糖蛋白浓度升高被认为导致血浆氯氮平-α-1-酸性糖蛋白结合增加,从而导致总氯氮平血浆浓度升高,而未结合浓度无明显变化。在这里,我们研究了α-1-酸性糖蛋白血浆浓度与氯氮平未结合分数之间的关系。
首先,将 25 和 60 μLα-1-酸性糖蛋白溶液(20mg/mL)加入氯氮平使用者的血浆样品(n = 3)(加标实验)。其次,在患者样本中评估α-1-酸性糖蛋白血浆浓度与氯氮平未结合分数之间的关系(患者研究)。样品通过液相色谱-串联质谱法测定。用配对 t 检验(加标实验)和未配对 t 检验(患者研究)分析数据。
加标实验表明,α-1-酸性糖蛋白加标 25μL 和 60μL 后,平均未结合分数明显降低(相对降低 28.3%,p = 0.032 和 43.4%,p = 0.048)。在患者研究中,与正常α-1-酸性糖蛋白(n = 20)样本相比,α-1-酸性糖蛋白升高(n = 6)的总氯氮平血浆浓度高 10%[525μg/L 比 479μg/L,平均差值为 47μg/L(95%置信区间 217 至 310),p = 0.72]。与正常样本相比,α-1-酸性糖蛋白升高的样本平均未结合分数低 26%[1.22%比 1.65%,平均差值为-0.43%(95%置信区间-0.816 至-0.0443),p = 0.03]。
加标实验和患者研究均表明,α-1-酸性糖蛋白血浆浓度升高与氯氮平未结合分数降低之间存在显著关联。未来的研究应包括临床数据,以检查这种关联是否具有临床相关性,提示需要调整氯氮平剂量。