Pollard E Morgan, Lamer Tim J, Moeschler Susan M, Gazelka Halena M, Hooten W Michael, Bendel Markus A, Warner Nafisseh S, Murad M Hassan
Division of Anesthesiology and Perioperative Medicine, Mayo Clinic, Rochester, MN 55905, USA.
Division of Pain Medicine, Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, Rochester, MN 55905, USA.
J Pain Res. 2019 Apr 30;12:1311-1324. doi: 10.2147/JPR.S186662. eCollection 2019.
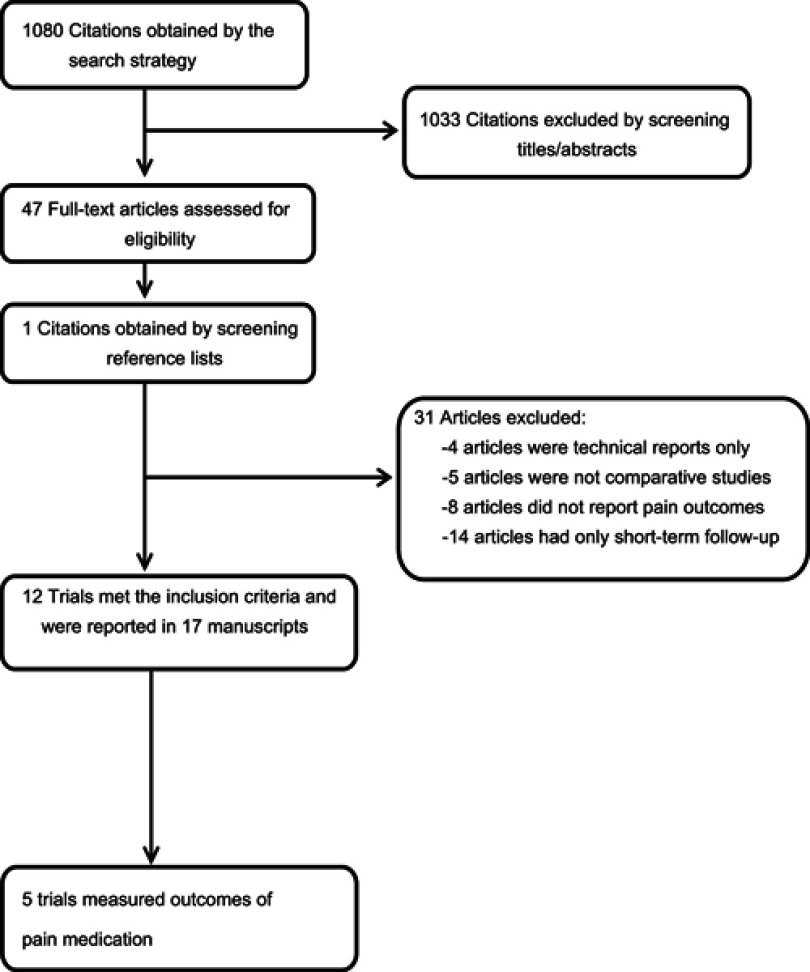
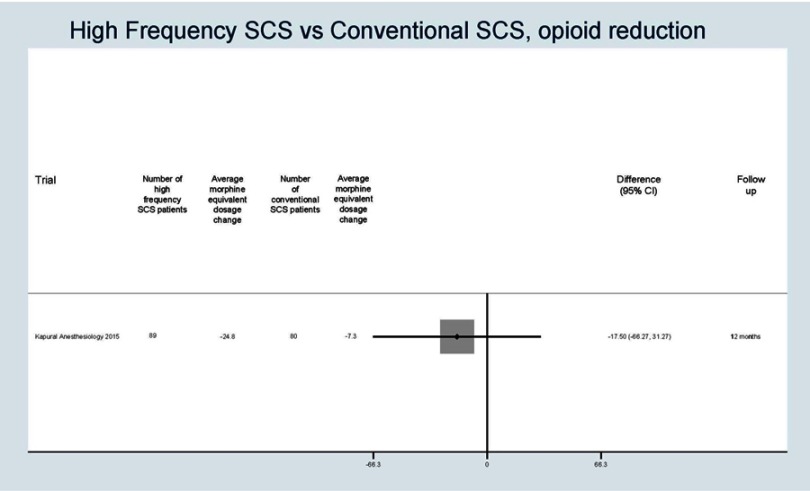
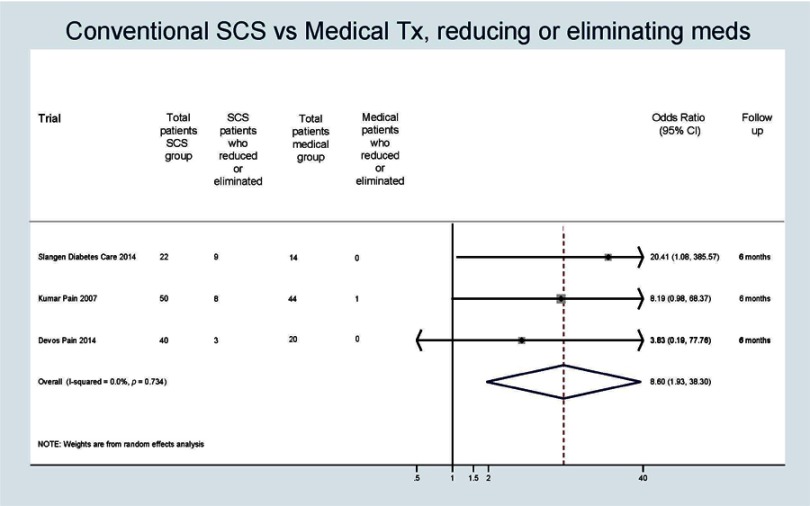
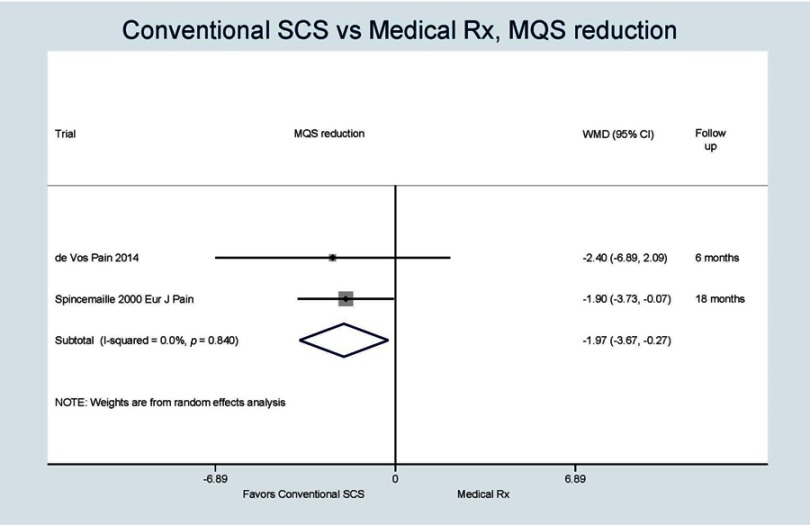
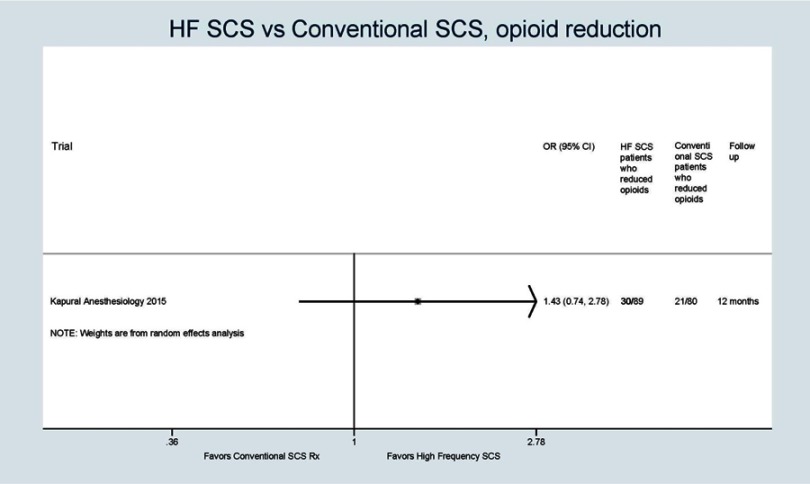
To synthesize the evidence regarding the effect of spinal cord stimulation (SCS) on opioid and pain medication reduction in patients with intractable spine or limb pain. A comprehensive literature search was conducted to identify RCTs of patients with chronic back and/or limb pain of greater than one year duration. Only comparative studies were included (ie, conventional SCS vs medical therapy, conventional SCS vs high-frequency SCS) and were required to have a minimum follow-up period of 3 months. Random effect meta-an alysis was used to compare the three interventions. Results were expressed as odds ratio (OR) or weighted mean difference (WMD) with 95% confidence intervals (CI). We identified five trials enrolling 489 patients. Three of the trials reported the results as a number of patients who were able to reduce or eliminate opioid consumption in the SCS vs medical therapy group. The odds of reducing opioid consumption were significantly increased in the SCS group compared to medical therapy (OR 8.60, CI {1.93-38.30}). Two of the trials reported the results as mean medication dose reduction as measured by the Medication Quantification Scale (MQS) in the SCS group vs medical therapy group. MQS score significantly decreased in the SCS group and not in the medical group (WMD -1.97, 95% CI {-3.67, -0.27}). One trial reported a number of patients in high-frequency SCS who were able to reduce opioids vs number of patients in conventional SCS group who were able to reduce opioids. Thirty-four percent of the patients in the high-frequency group and 26% of the patients in the conventional SCS group were able to reduce opioid consumption; however, there was not a significant difference between groups (OR 1.43, 95% CI {0.74, 2.78}). This trial also quantified the opioid reduction in morphine equivalent dosage (MED). In the high-frequency SCS group, average MED decreased by 24.8 mg vs average MED decrease of 7.3 mg in the conventional SCS group. Again, the difference between groups did not reach statistical significance (-17.50, CI {-66.27, 31.27}). In patients with intractable spine/limb pain, SCS was associated with increased odds of reducing pain medication consumption. However, results should be treated with caution as available data were limited, and clinical significance of these findings requires further study.
综合有关脊髓刺激(SCS)对顽固性脊柱或肢体疼痛患者减少阿片类药物及止痛药物使用影响的证据。进行了全面的文献检索,以确定针对慢性背痛和/或肢体疼痛持续时间超过一年患者的随机对照试验(RCT)。仅纳入比较研究(即传统SCS与药物治疗、传统SCS与高频SCS),且要求最短随访期为3个月。采用随机效应荟萃分析比较这三种干预措施。结果以比值比(OR)或加权平均差(WMD)及95%置信区间(CI)表示。我们确定了五项纳入489例患者的试验。其中三项试验报告了SCS组与药物治疗组中能够减少或消除阿片类药物使用的患者数量。与药物治疗相比,SCS组减少阿片类药物使用的几率显著增加(OR 8.60,CI {1.93 - 38.30})。两项试验报告了SCS组与药物治疗组按药物量化量表(MQS)测量的平均药物剂量减少结果。SCS组的MQS评分显著降低,而药物治疗组未降低(WMD -1.97,95% CI {-3.67,-0.27})。一项试验报告了高频SCS组中能够减少阿片类药物使用的患者数量与传统SCS组中能够减少阿片类药物使用的患者数量。高频组34%的患者和传统SCS组26%的患者能够减少阿片类药物使用;然而,两组之间无显著差异(OR 1.43,95% CI {0.74,2.78})。该试验还以吗啡当量剂量(MED)量化了阿片类药物减少情况。在高频SCS组,平均MED减少24.8 mg,而传统SCS组平均MED减少7.3 mg。同样,两组之间的差异未达到统计学显著性(-17.50,CI {-66.27,31.27})。在顽固性脊柱/肢体疼痛患者中,SCS与减少止痛药物使用的几率增加相关。然而,由于现有数据有限,结果应谨慎对待,这些发现的临床意义需要进一步研究。