Department of Epidemiology, Rollins School of Public Heath, Emory University, Atlanta, GA.
Department of Gynecology and Obstetrics, School of Medicine, Emory University, Atlanta, GA.
Am J Obstet Gynecol. 2019 Oct;221(4):347.e1-347.e13. doi: 10.1016/j.ajog.2019.05.034. Epub 2019 May 25.
Relatively little is known about the frequency and factors associated with miscarriage among women living with HIV.
The objective of the study was to evaluate factors associated with miscarriage among women enrolled in the Women's Interagency HIV Study.
We conducted an analysis of longitudinal data collected from Oct. 1, 1994, to Sept. 30, 2017. Women who attended at least 2 Women's Interagency HIV Study visits and reported pregnancy during follow-up were included. Miscarriage was defined as spontaneous loss of pregnancy before 20 weeks of gestation based on self-report assessed at biannual visits. We modeled the association between demographic, behavioral, and clinical covariates and miscarriage (vs live birth) for women overall and stratified by HIV status using mixed-model logistic regression.
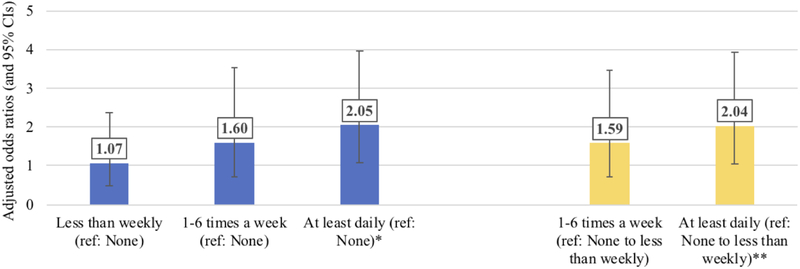
Similar proportions of women living with and without HIV experienced miscarriage (37% and 39%, respectively, P = .638). In adjusted analyses, smoking tobacco (adjusted odds ratio, 2.0), alcohol use (adjusted odds ratio, 4.0), and marijuana use (adjusted odds ratio, 2.0) were associated with miscarriage. Among women living with HIV, low HIV viral load (<4 log10 copies/mL) (adjusted odds ratio, 0.5) and protease inhibitor (adjusted odds ratio, 0.4) vs the nonuse of combination antiretroviral therapy use were protective against miscarriage.
We did not find an increased odds of miscarriage among women living with HIV compared with uninfected women; however, poorly controlled HIV infection was associated with increased miscarriage risk. Higher miscarriage risk among women exposed to tobacco, alcohol, and marijuana highlight potentially modifiable behaviors. Given previous concern about antiretroviral therapy and adverse pregnancy outcomes, the novel protective association between protease inhibitors compared with non-combination antiretroviral therapy and miscarriage in this study is reassuring.
目前对于感染 HIV 的女性流产的频率和相关因素知之甚少。
本研究旨在评估参与妇女艾滋病研究机构(Women's Interagency HIV Study)的女性中与流产相关的因素。
我们对 1994 年 10 月 1 日至 2017 年 9 月 30 日期间收集的纵向数据进行了分析。符合以下条件的女性被纳入研究:至少参加了 2 次妇女艾滋病研究机构研究访问,并在随访期间报告怀孕。流产定义为根据每两年一次的访问中自我报告的妊娠在 20 周前自然丢失。我们使用混合模型逻辑回归模型,对总体女性和按 HIV 状态分层的女性,对人口统计学、行为和临床协变量与流产(与活产相比)之间的关系进行建模。
感染和未感染 HIV 的女性流产比例相似(分别为 37%和 39%,P=0.638)。在调整后的分析中,吸烟(调整后的优势比,2.0)、饮酒(调整后的优势比,4.0)和使用大麻(调整后的优势比,2.0)与流产有关。在感染 HIV 的女性中,低 HIV 病毒载量(<4 log10 拷贝/ml)(调整后的优势比,0.5)和使用蛋白酶抑制剂(调整后的优势比,0.4)与未使用联合抗逆转录病毒治疗相比,可降低流产风险。
与未感染的女性相比,我们没有发现感染 HIV 的女性流产的几率增加;然而,HIV 感染控制不佳与流产风险增加有关。烟草、酒精和大麻暴露的女性流产风险较高,突显了潜在的可改变行为。鉴于先前对抗逆转录病毒治疗和不良妊娠结局的担忧,本研究中蛋白酶抑制剂与非联合抗逆转录病毒治疗相比与流产之间的新的保护关联令人欣慰。